I have done more traveling than I probably should have in January and February between the US, the Middle East and various places in Europe.
One of the constant themes was the place of a regulatory regime in the world and how to calibrate the regulatory system just right in the way that it meets both the requirements of society and industry the best. I attended very interesting discussions on this subject in Dubai at the Mecomed RAPS MEA event on 30 January.
At the Lab Quality Days in Helsinki (a conference which I highly recommend if you’ve not attended so far) the red thread was how to calibrate the IVDR and EU horizontal legation like the AI Act in a way that you create a predictable and reliable regulatory system, in which we did not succeed that well in Europe. This lead more and more companies to abandon the historic ‘Europe first’ strategy.
The last IMDRF meetings were flush with talk about international reliance, leading to more and more regulatory convergence. It breaks my regulatory heart to see that international developments seem go the other way now.
International reliance assumes a two way street and a willingness to be a good example by setting standards others want to follow and following them yourself as well.
In that regard we have overshot the mark in Europe with our over-engineered medical devices regulations with its overly complex transitional regime and our complex layers regulatory lasagna piled on top. At the same time the system is decentralised and under-resourced both on EU and national levels. Reality is showing that this has led to a rather over engineered regulatory system that has difficulties delivering on its promise.
I have expressed doubts in my last blog about the course taken by the current US administration, the outlines of which seems to become clearer and clearer as the US seems to have opted for a very rigorous stripping down of its institutions, especially where they are active internationally (or manage nuclear weapons), and for a zero sum perspective on international relations, including alianating allies wherever possible.
The question now is how the US will fare in international reliance with this approach and how many countries will (continue to) see the US as a reliable source of rule based thinking and two-way relations.
If we look at the WHO regulatory reliance definition (“The act whereby the regulatory authority in one jurisdiction takes into account and gives significant weight to assessments performed by another regulatory authority or trusted institution, or to any other authoritative information in reaching it own decision.”) you can immediately see how this will be problematic for the US. These days nobody is bigger than the rest of the world no matter how hard you try.
How this will translate to devices policy both national and international is still not completely clear but I am not optimistic based on developments so far. For example, what will all of this mean for the US participation in the IMDRF? In this regard it’s encouraging that the Commission has announced that it will step up its international activity, which hopefully will include a more active participation in the IMDRF.
This means that Europe is in a great position to restore its position as a jurisdiction of choice for regulatory approval and regulatory reliance, IF it can get its act together. If.
EU competitiveness compass, targeted evaluation and implementing acts
How will the EU get its act together? As I’ve blogged earlier this year by means of a strategy of quick anti-bureacracy wins and targeted changes to the MDR and the IVDR.
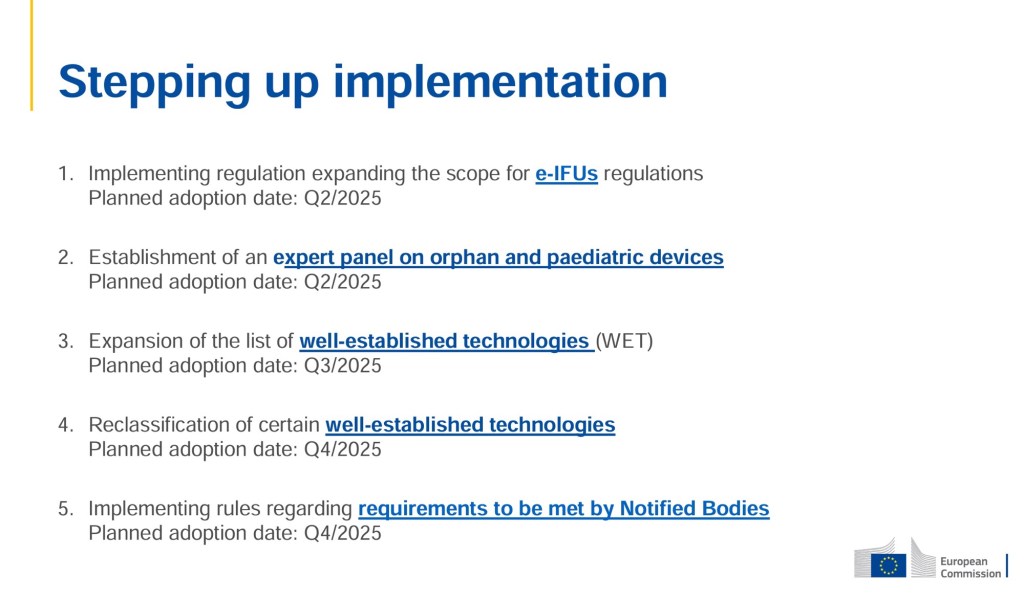
I have already seen the Commission announce the first changes to the MDR and IVDR by means of regulatory and non-regulatory actions (the quick wins):
Implementing regulation expanding the scope for e-IFUs regulations
Establishment of an expert panel on orphan and paediatric devices
Expansion of the list of well-established technologies (WET)
Reclassification of certain well-established technologies
Implementing rules regarding requirements to be met by Notified Bodies
The Commission is still on track to present a proposal for legislative changes later this year. The member states also have the option to finally deliver on their ideas set out in the MDCG 2022-14 position paper.
In a larger context at EU economy level the Commission has presented its Competitiveness Compass for Europe, which, if it will really be rolled out as promised in this communication (COM 2025 (30) final), should lead to significant simplification and deregulation of EU law and a reduction of ‘regulatory ratchet’ – the politically correct term for regulatory lasagna. Even medical devices are explicitly mentioned in the Compass, in relation to simplification of regulatory requirements.
The Compass is functionally built around three pillars and five horizontal cross-cutting measures. Other than from a regulatory perspective the medical device industry may find it interesting that the EU wants to make it much easier for startups to scale making access to cross-border investments much easier, among which by means of the “28th regime”. This is a a single, harmonised set of EU-wide rules that innovative companies can benefit from wherever they invest and operate in the Single Market. A Data Union Strategy should improve and facilitate secure private and public data sharing, simplify the regulatory regime and its application, and accelerate the development of new systems or applications.
While this all sounds totally super on paper, I still remember earlier initiatives in 2008 that were supposed to make the EU the most competitive economy in the world and at the moment we’re not there yet.
Like the US at the moment, the EU is its own worst enemy in the execution of policy and regulation. The EU is divided among its member states and encroached upon by populists that do not believe in the European project but would rather take their country back to the early fifties when everything was better, people still said hello to each other in the street, life was simple, and the sun was shining every day.
The biggest challenge for the EU will be to rally the member states behind this compass and to do much better in convincing the population what the benefits of the EU are.
It’s frankly ridiculous for example how the EU negotiates international trade agreements that are subsequently torpedoed wholly or in part on national level because of local interests of groups of people that choose not to see the bigger picture based on EU hostile desinformation. This does nothing for the reliability of the EU in the world.
What did I find interesting last weeks?
The competitiveness compass of course. Go Europe!!
There was an updated notified body Q&A document (MDCG 2019-6 Rev. 5) from the MDCG with rather interesting guidance on structural dialogues (section I.6) and a possible (and non-exahustive) list of structured dialogue topics. This means that every notified body should be willing to open a dialoogue on these matters without deflecting it out of hand with a ‘this is consultancy’ statement. It will force notified bodies to think about more about how not to be the department of ‘no’ but rather of ‘it’s better to approach it this way’. Manufacturers, for their part, should take care not to ask open ended questions and expect the notified body to tell them exactly how to comply with the requirement, because that would be consultancy. It will also assist notified bodies in being more service minded for the overall benefit of society, also a nice benefit.
The Commission presented an overview of five implementing acts at the Mecomed RAPS MEA conference on 30 January that it is working on with a view to fix aspects of the MDR and IVDR quickly, among others an implementing act on eIFU (expected, but scope still unclear) and (this was what I found especially interesting) an implementing act on harmonization of notified body procedure. This would fit very well in the industry advocated ‘harmonization through centralization’ concept – so watch that space as the implementing acts become available for consultation. Also, interestingly, the Commission will increase international cooperation.
We are waiting for the opinion of the Advocate General in a very interesting borderline case at the EU Court, which is about one of my borderline hobby horses: weak reversible bonds between substances and bacteria, such as Van der Waals forces. Their unfortunate mentioning in MDCG 2022-5 has led to a situation where too easily products that work based on Van der Waals forces are deemed to have a pharmacological mode of action without any discussion of actual science, which (unfortunately) is a no-so-scientific policy overreach. Why? Because if all Van der Waals bonds would be a pharmacological mode of action this would make most of the most of the weak bonds that keep the fabric of the physical world together pharmacological – and that’s a huge oxymoron. The ubiquitous nature of Van der Waals forces disqualifies them as pharmacological interactions. Van der Waals forces occur between all molecules that come into close proximity – they’re present between water molecules in a glass, between proteins in your body, between air molecules, and even between your fingers and the surface you touch (that’s hopw geckos stick to walls). They arise simply from temporary fluctuations in electron distribution that create momentary dipoles. If we were to classify Van der Waals forces as pharmacological interactions, we would need to consider: – Every protein-protein interaction in your body as pharmacological; – Every time water molecules interact with cellular components as pharmacological; – Every instance of membrane lipids associating with each other as pharmacological; and – Even the adhesion of dust particles to surfaces as pharmacological. This would make the term “pharmacological interaction” lose its meaningful distinction from basic physics. The essence of pharmacology is the study of specific, targeted interactions that produce defined biological effects. A pharmacological interaction needs to be selective and purposeful – like a key fitting into a lock – rather than a universal background force that affects all matter. This is why we should rather reserve the term “pharmacological interaction” for specific binding events that trigger defined biological responses, while recognizing Van der Waals forces as one of several physical forces that contribute to, but don’t themselves constitute, these interactions. I am not alone in my criticism regarding MDCG 2022-5. Member States Italy and Germany have also concluded that the concept of pharmacological mode of action set out in it is not sufficiently precise to be helpful as guidance. Hopefully the EU court will be smart about this.The AG is not yet the final judgment of the court but the EU Court follows its AG in the majority of the cases. I am watching that space!
Withdrawal of the AI Product Liability Directive – the Commission withdrew the proposal for the AI Product Liability Directive because there was no foreseeable agreement in the legislative procedure. One of the main bones of contention was the eroded burden of proof of the claimant in case of AI products that formed the core of the directive. This will have implications for medical devices that implement AI or are an AI system themselves as these will remain subject to general the general product liability directive, see the Commission’s work programme and annexes.
Where to meet me?
RMD 2025 in Brussels on 24-25 February on changes to the MDR and IVDR – always very interesting and high quality with great access to leading experts
Irish MedTech article 10a workshop on 5 March in Limerick
RAPS Netherlands Chapter in Leuven on in-house produced devices on 5 March. The RAPS NL Chapter is very active and has a very high quality of information exchange and networking. If you work in devices RA/QA and speak Dutch, RAPS NL will be indispensible.
Happy new year everyone! I hope you had a good rest over the holidays because 2025 will be interesting.
I am planning to revive this blog this year and hope to put new energy in it by making it more periodical with smaller bits of information and shorter analysis. You will still get my unique perspective on things and I’ll probably not be able to help myself so will probably occasionally write more in depth stuff anyway. For the actualities and the occasional arguments with others, follow me on LinkedIn.
2025 will be interesting with short term changes to the MDR and IVDR
Everybody and their mother and then some other people even has been clamoring for changes to the structure of the MDR and the IVDR. The Commission has indicated that it will pursue measures in the short term intended to combat bureaucracy slowing down the system (such as the still not optimal functioning of structural dialogues). Member States / MDCG can be part of this solution by just implementing all points of MDCG 2022-14 and facilitate notified bodies in this regard with uniform instructions and otherwise just let the Commission do its job.
The Commission is planning to present a package of proposals more structural changes later this year (Q4), the targeted evaluation. These will be based in the fact finding exercise conducted in the second half of 2024 (of which the results are still to be published), the call for evidence currently open and may be inspired of course by the many helpful white papers, position papers, Parliament joint resolution and EPSCO paper and other initiatives. You can still submit comments and wishes in the Commission’s public consultation open until 25 March 2025.
If there is one structural change that I would personally favor it would be more accountability of notified bodies, legal review of all of their decisions by analogy to article 51 (2) MDR and more external harmonisation of their procedures, as this would force notified bodies to be more the solution to the problem than part of the problem. Let’s not forget that notified bodies wield delegated state power that enables them to unilaterally determine the rights and obligations of citizens, with at the moment basically zero accountability as this is not built into the system. What this sort of control could look like has been set out in the BVMed and VDGH white paper and Peter Liese initiative. Exercise of state authority without effective accountability, that does not sound very constitutional and I can assure that much can be improved there.
In the mean time we had the Dragi report in the EU and we have a new Commission with new plans. We will need to see how the new EU Commissioner for Health attacks the MDR and IVDR. At this point I am still wondering how this is going to happen with the degree of understaffing of the devices unit at DG Health that has a headcount of less than 10 people. It’s a big burden on a small team and I have said more than once that these people deserve great respect for what they manage to do with such a small team. If I were in charge my first action would be to properly resource this unit. Maybe someone could calculate the external costs to society of this unit being under-resourced? I bet that this these are much higher than tripling the headcount, apart from the moral hazard of not properly resourcing the Commission for devices policy.
Under-resourcing seems to be a general theme: I keep experiencing how difficult it is for EU medtech startups to secure EU based funding and having to spend a lot of the funding from whichever source on often preventable mistakes in regulatory strategy and/or pretty steep notified body fees. This is also one of the themes in the Dragi report.
Let’s not become an open air museum of bad choices in Europe!
US and EU political developments
The FDA has been running circles around the EU regulatory system for the last years with market access procedures that worked a lot better, were way most cost effective and encouraged innovative devices to the market earlier than possible in Europe. The FDA did really well in this regard.
But will they we able to keep this up during the new administration? We will need to see how the FDA and its procedures are affected by the new administration’s plans with downsizing and gaining more direct influence over independent government institutions.
Maybe the regulatory pendulum will swing back to EU once more after all the changes planned to the MDR and IVDR for 2025 and the Union will be called one big clinical trial for the US again. Who knows!
Interruptions and discontinuations reporting as of 10 January
The new obligation under the MDR and IVDR to report interruptions and discontinuations of supply enters into force on 10 January. We now have Commission Q&A, a reporting form and still a lot of remaining questions. A lot these were asked at the webinar that I was part of together with Bassil Akra on 17 December 2024. I have emailed everyone by now that had questions that were not answered at the webinar. You might still be able to get the recording via Sean Smith of Medtech Leading Voice.
My take away is that the legal dimensions of this change are still not well understood by manufacturers and especially not be the supply chain, but also not by competent authorities. Manufacturers and distributors often have no idea how shortage reporting may impact their distribution, tender and supply agreements. For example, a shortage report may trigger an anticipatory breach or other right of the other party. Regarding competent authorities it will be interesting to see if they understand what it means in the Commission Q&A about article 10a that article 109 MDR/102 IVDR apply, meaning that the information repored to them is confidential. Yet, I have for example seen competent authorities argue that local freedom of information regulation trumps article 109 MDR / 102 IVDR and without much qualms disclose information from vigilance reports pursuant to freedom of information requests of parties working on product liability claims. Why is this kind of policy problematic? Because you cannot be sure that what you report in confidence stays confidential and will not be used against you. That makes reporting or full reporting risky and leads to a chilling effect on reporting. This will help nobody to achieve their goals. We’ll also have to see what any national enforcement policy will look like and if national competent authorities have the capacity to review the reports filed in any meaningful level of detail anyway.
If you have more questions, or need help taming the beast of article 10a, let me know.
By the way, there will be a full article on article 10a coming (in English) in the German legal journal MPR by my colleague Judith de Wilde and me. Watch that space!
What (else) did I find interesting last month(s)?
As a new feature on this blog I decided to add a section to blogs about what I found interesting last month(s), as this may signal developments interesting to others too.
Significant changes and mergers
Mergers and significant changes keep causing headaches and costing (a lot) money unnecessarily. First, application of the concept of ‘significant change’ in article 120(3c) (b) MDR by notified bodies in the context of mergers remains a source of controversies. While the section on administrative changes in MDCG 2020-3 Rev 1 that mentions ‘mergers’ are allowed as administrative changes, notified bodies often get hung up on the clarification in footnote 17 that the result of a merger must be that the manufacturer legal entity must remain after the merger. This has been added to clarify that asset transfers that require new certificates to be issued in the name of a new legal entity are not allowed. Notified bodies will tend to interpret this as that mergers between legal entities in which the manufacturer entity is merged into the acquiring legal entity trigger a substantial change, while this is clearly not intended by the Commission (see also Q&A on Regulation 607/2023, question 9.2).
I have found that notified bodies are typically not very good at understanding what a merger is and then cling to misinterpreting the literal text of footnote 17. This causes sometimes quite severe damage and costs for the manufacturer and/or the acquirer. It may lead to unnecessary cancelling the legacy device certificate, causing to the devices in scope of the cancelled certificate to be no longer available to the market. Yes, this is precisely what was not intended by the EU legislator with the legacy devices regime. Notified bodies do not seem to understand the existential crisis that they can put a company in by being unpredictable, slow or unreliable with respect to merger activity.
In my experience with this, contact persons at the notified bodies were without exception unqualified for a meaningful discussion that had any depth beyond the literal text of the MDR or Commission/MDCG guidance (no legal understanding or training, nor any recourse to the notified body’s legal department), which is disturbing and puts entirely needless pressure on the relationship between the manufacturer and the notified body. This reflects badly on the EU regulatory system.
My pro tip for notified bodies would be to clarify their understanding of the concept of significant change in merger scenarios with their competent authority, immensely up their game in discussion of a potential significant change in a merger scenario with a manufacturer and make sure that their legal department is available to assist front line staff that is basically never qualified for legal matters immediately to prevent unnecessary escalation.
Manufacturers and their acquirers, for their part, should never assume that the notified body will intuitively understand what a merger and its effect is (this includes basic corporate house keeping within the corporate group – never dissolve / merger a legal entity without talking to regulatory first), should explain how it is not a significant change, have this confirmed by the notified body in advance and (important) have a very good paper trail of this before implementing the merger. Be ready to escalate to the notified body’s competent authority because they may be on your side more often than you think. And MDCG, please please please why not just write this down better? It would save so much agony and costs and improve the impression of predictability and reliability of EU medical devices law.
Batteries regulation
The Batteries Regulation keeps people very busy, as the first major phase in date (18 August 2024 for CE marking of batteries) has passed now. The Batteries Regulation is horizontal EU legislation and applies regardless of MDR or IVDR compliance, which is something many companies in the devices do not realise. Non-compliant battery leads to a non-compliant device, and there is your conundrum. We spent a lot of time in Q4 2024 helping manufacturers of medical devices and IVDs figure out how to work with the Batteries Regulation.
Did you know that even cybersecurity is a thing for batteries? If the battery in your device has battery management software that can talk to the outside world somehow, you have a cyber security risk to manage (also as part of the device’s cyber risk management – see MDCG 2019-16, Annex II regarding battery depletion as a result of external unauthorised acces).
Would you like to go on a Battery Regulation safari with me and my battery specialist colleague Jilles like some of the biggest medtech companies have already done and found interesting? Let me know!
Swixit reversal?
It was not in the press much, but a Swixit reversal may be in the works. Not immediately, but the EU and Switzerland have taken steps again to revisit the integration of Switzerland into the EU internal market, which would mean that mutual recognition of CE marking and Swiss notified bodies might be back on the table. It’s still early days and the current package is not the same as the comprehensive Institutional Framework Agreement that turned out to be more than Switzerland could process politically, but negotiations seem to go the right way. Basically we are back to good old MRA times and a new MRA for MDR and IVDR would be very logical (and has the warm support of industry).
What could that mean for the plan of Switzerland recognise FDA approved devices? Good question! First, this plan has still not been implemented. Secondly, given these developments it might never be.
Watch the negotiations between the EU and Switzerland as the MRA and its MRA annex are filled in in the coming months.
eIFU regulation amendments coming – eIFU for all professional use devices
After the consultation last year about extending the eIFU regulation to other professional use devices the Commission has now announced that it plans to adopt the new implementing regulation in Q2 2025, which will allow to issue electronic instructions for use for all medical devices intended for exclusive use by healthcare professionals. We are still very much in the stone age in Europe on eIFU, since the underlying assumptions to the current eIFU regulation are that basically nobody has reliable access to internet and that everyone saves their paper IFUs for reference use. By now all these underlying assumptions have proven wrong and outdated, and it’s time for a thorough update.
Although this still does not seem to be in the stars for the upcoming update, many other jurisdictions allow eIFUs for lay users as well, and there is no reason for the EU not to do so either given the experiences in other jurisdictions. While the outcome of the last consultation has not been published yet, I’ve seen the results and even professional users overwhelmingly agree that this would be a good idea for lay users. In fact, let’s not forget how only providing paper IFUs disadvantage people with disabilities and are even contrary to other EU law intended to make life easier for persons with disabilities by obliging IFUs for products to be provided in multiple sensory channels. Who use a lot of medical devices you ask? Indeed: persons with disabilities, generally. Let stop limiting their autonomy with these unjustifiably outdated eIFU rules.
Reclassification of WET
One of the problems with well-established technologies is that you would think they could do with some less strict oversight (especially on the class III and IIb classes). The Commission aims to reclassify certain well-established technologies, for which the application of the general classification rules in Annex VIII of the MDR is not proportionate to the devices’ nature and respective (limited) risks, with a new implementing act planned for Q4 2025.
New consolidated version of MDR published
Many people don’t understand how Eur-Lex works and get their MDR and IVDR text versions wrong. The most recent consolidated version which includes all the last changes have just been published for the MDR but not yet for the IVDR (which is still in the consolidated version of July 2024). Understanding how Eur-Lex works and how to use this incredibly versatile tool is a very good investment of your time (next to reading the Blue Guide). If you ever need to recruit or vet regulatory staff or consultants with EU capabilities, ask them two these things: show me how Eur-Lex works and have you read the most recent version of the Blue Guide? In case of unsatisfactory answers, these are not the people you’re looking for.
Conference appearances planned
A new year, new conferences. What am I up to? Currently I’m planning to be at
The OSMA Winter 2025 meeting in Orlando 21-23 January – if you’re into orthopaedics (and SeaWorld), come and meet me there!
EUCROF Copenhagen 2-4 February, because clinical investigation and performance evaluation is and remains a tricky subject. Pharma companies for example routinely forget that assays used in clinical trials are likely to IVDR controls too. Why would that be relevant? Well, how about all of your clinical trial data collected with the use of these assays not being valid – that should get your management’s attention.
Lab Quality Days in Helsinki 6-7 February speaking about AI development in-house by health inastitutions and about the regulatory lasagna created by the AI Act. If you are doing anything with AI in lab setting, this will be your go-to event.
The RAPS EU Convergence in Brussels 13-16 May – I will be presenting about MDR/IVDR and their relation to environmental / Green Deal regulation in the EU (like the Batteries Regulation for example) – many attendees found this very interesting in at the EU RAPS Convergence in 2024.
MedTech Summit in Berlin 16-20 June, where I will be presenting a regulatory forecast “Locking Down the Law: BVMED-VDGH, MTE White Papers, Peter Liese Proposal, Targeted Evaluation – Where is This All Going?”
So if you’re interested in meeting me, meet me at these international events! Others are in the works and I’m planning a boatload of webinars for this year as there is so much to talk about.
And: this year will likely see the third edition of The Enriched MDR and IVDR, to which I’ve added presently 200+ additional pages of substantive content and of which I’ve revised and updated a lot of content too (that was a lot of work that did not go into this blog).
Why should we watch what happens in German Parliament?
The Council is one of the three important institutional actors in the legislative procedure for amendments to the MDR, the co-decision procedure. And Germany is one of the most active and heavyweight Member States in the Council when it comes to medical technology matters so what Germany wants with the MDR will carry a lot of weight.
We also know now what the European Parliament wants (Peter Liese’s initiative), and we also know that the Commission is keeping its cards close to its chest for the moment although we do know that also the Commission wants amendments to the MDR in the short term (the planned ‘targeted evaluation’) and may well be working on those already.
The Bundestag session will take place tomorrow from 14:45 to 15:45 CET. You might be interested in the position papers (Stellungnahmen) filed for this session (including mine), which can all be conveniently downloaded here. For those interested, the session in the Bundestag has a public live stream that you can watch (in German).
What you will see happening tomorrow may be another important step in how the MDR and IVDR may change soon.
Convergence happening
As I’ve recently posted on this blog, there is a momentum of converging of positions building up. For example, the Peter Liese initiative was generally received quite well by industry as I’ve been told by several people. But we cannot fix the MDR alone as the IVDR suffers from the same issues, as I have argued in my position paper sent in for Parliament session tomorrow.
This momentum will culminate in the short term and will lead to targeted but significant revisions of the MDR and IVDR to fix the bigger inefficiencies and improve these regulations by building on the solid foundations that are already there with the experience gained since 26 May 2017. My guess is that we will see this happen early 2025.
For me personally the most important points as a legal and regulatory expert are that
the governance system for the MDR and IVDR needs revision to become more centralised and less bogged down by individual member state / notified body hobby horses and hangups; and
principles of good administrative practice need to be implemented in the system to ensure that the delegated state powers of granting market access through conformity assessment are exercised responsibly and are subject to standard legal review as befitting in a democratic society.
Everyone is part of the solution
Everyone needs to be part of the solution to make the system work because as things go the MDR and IVDR are underdelivering in a completely preventable way as they are suffering from problems caused by policy choices, both on EU and national level (notably those underlying the transitional regime and Member States’ resourcing of the implementation and notified bodies re-notification). The good part about this type of choices is that they can be remedied. Because let’s face it: we are all (potential) patients and have dear ones that are (potential) patients, and we would like a devices regulatory system that lives up to its promise. And then there is the geopolitical dimension: why would the EU, who prides itself on being world champion in setting the bar for regulation, inflict this crisis of healthcare and innovation upon itself if it is entirely preventable? It’s time for everyone to step up and do better. Because who has two thumbs and can be part of the solution? Yes that’s right – that is you. You could start right now.
The MDR and IVDR are now in force for seven (7) years, and they are not in good shape.
I think it is safe to say that they did not deliver on their promise of a better, more streamlined and more SME and innovation friendly regulatory system.
Deadlines keep being moved, patchwork happens here and there. But it is still not a world-class regulatory system – essential parts like Eudamed are not even finished yet. Innovation is fleeing to other jurisdictions and hospitals complain about shortages of devices. This is not a good place to be, and certainly not to stay.
Legacy devices
Today is an important day under the MDR, as the era of legacy devices truly starts. The manufacturers that do not have an MDR application in the works by today will lose existing legacy device benefits.
We have now truly entered the era of legacy devices – an area in which is ever harder for the outside world to understand. Many of the non-Union jurisdictions that attach importance to CE certificates for local registration are finding it more and more complicated to understand if a certificate is actually valid or not after Regulation (EU) 2023/607 created the MDR legacy devices regime that we have today. Having legacy devices certificates is of course better than not having any certificates but I often see that manufacturers do not really know what it entails.
First, there is the issue of no significant changes. That’s right, the device’s design and intended purpose are essentially frozen until the MDR or IVDR certificate drops. That means that competitors that get their MDR or IVDR certificates earlier can outcompete you with new features that you are not able to implement yet.
Secondly, the notified bodies have until end 2027 or 2028 (depending on risk class) to finish the conformity assessment and even if they don’t by then this has no legal consequences. So there is a clear incentitve to be MDR or IVDR for the manufacturer to be CE marked as soon as possible. In that regard it is strange that notified bodies are reporting a drop in applications, both for MDR and IVDR. There is no obligation for the notified bodies to finish as soon as possible unfortunately.
Also, it is not encouraging at all that the number of application refusals is increasing, with refusal for incomplete applications and applications outside the scope of designation of the notified body accounting for the two biggest grounds of refusal. These grounds for refusal should normally be avoidable, and yet they happen more and more.
In-house produced devices
It’s also an important day under the IVDR, because all except the last of the requirements for in-house produced devices in article 5 (5) IVDR become applicable. Only the justification requirement for the use of an in-house produced device still needs to become applicable on 26 May 2028.
While the MDCG has issued guidance (MDCG 2023-1) on the subject, this guidance is really broad in some areas and shows divergence in policy (or absence thereof) between member states. It seems that most member states are just waiting with local policy until they have an idea of the likely level of compliance in their respective markets. Where member states do express themselves I’ve seen interesting things, such as for example statements that cross-border testing is not allowed under article 5 (5) IVDR – excuse me? Health institutions can provide cross-border medical services to patients in the EU but not testing services? That would be very much at odds with the internal market.
The health institutions, for their part, have a hard job complying – especially the hosptial labs that are invariably under-resourced to do the extra work required under article 5 (5) IVDR.
So we seem to be entering into a kind of wild west phase for in-house produced devices. We have rules but scattered compliance and little enforcement.
The Council is expected to approve this on 30 May after which it will be published and enter into force somewhere in June most likely. The provision about supply interruption will enter into force six months after entry into force of the amendment, so this autumn. Manufacturers should be ready for this.
Although the proposal started out as targeting only interruptions of supply of a device but the version voted on by the Parliament additionally included discontinuation of supply of a device. As the proposal currently stands:
“a manufacturer [that] anticipates an interruption or a discontinuation of the supply of a device, other than a custom-made device, and where it is reasonably foreseeable that such interruption or discontinuation could result in serious harm or a risk of serious harm to patients or public health in one or more Member States, the manufacturer shall inform the competent authority of the Member State where it or its authorised representative is established, as well as the economic operators, health institutions and healthcare professionals to whom it directly supplies the device, of the anticipated interruption or discontinuation.
The information referred to in the first subparagraph shall, other than in exceptional circumstances, be provided at least 6 months before the anticipated interruption or discontinuation. The manufacturer shall specify the reasons for the interruption or discontinuation in the information provided to the competent authority.”
There will also be additional obligations for economic operators: all importers, distributors and other economic operators involved (e.g. procedure pack or system composers) economic operators who have received the information from the manufacturer or from another economic operator in the supply chain shall, without undue delay, inform any other economic operators, health institutions and healthcare professionals to whom they directly supply the device, of the anticipated interruption or discontinuation.
This means that manufacturers will need to do an impact assessment with an at least 6 months horizon at least that looks at individual Member States in the Union if they plan to discontinue or temporarily stop supply of a CE marked device. And then tell everybody and their mother about it if this may create issues in one or more member states. Distributors and importers in the Union need to establish processes to inform the supply chain downstream as well.
I understand that the MDCG is working on guidance about how to apply this provision, which is a good idea as it is very vague. My own legal experience with broadly and vaguely drafted security of supply information obligations is not good.
I am litigiating several cases in relaton to medicines where companies were find for not complying with quite unclear and broadly worded similar requirements, I hope we can avoid this in devices. In the meantime these rules for medicines are being amended to become much more sophisticated in the review of EU pharmaceutical law. Why has the legisalator not looked at the experience gained in this sector? Your guess is as good as mine.
What’s next?
The Commission has announced in January when it made the propsal that is now nearing the end of the legislative pipeline that it will pursue further amendments to the MDR and IVDR to fix ongoing problems. The European Parliament also announced when it had voted for the latest amendment on 30 April 2024 that this would not be the end of amendments to the MDR and IVDR.
One of the most recent steps is that Peter Liese, member of the European Parliament and long since involved with the MDR and the IVDR, has forwarded a proposal for Parliament suggested changes to the European Commission, as was made public on a press conference on 17 May. I had the honour to be retained by Mr. Liese’s office to serve as external expert for developing this proposal.
The European Parliament does not have the right of initiative for amendments to legislation so this is not an actual pending legislative proposal now. However, Parliament can of course seek support within the Commission for this idea so the Commission may decide to table a proposed amendment for the Council and the Parliament in a legislative procedure that includes the Parliament’s ideas because it increases the chance of success and speed of the proposal. I understand this is exactly what Mr Liese has been doing.
“The Commission will already start in 2024 its preparatory work for a targeted evaluation of the legislation on medical devices. The evaluation should assess how the legislation is affecting the availability of devices, in particular for devices with specific characteristics (e.g. paediatrics, orphan, innovative devices). In the assessment, special attention may also be given to costs and administrative burdens stemming from the implementation of legislation, especially for SMEs.”
The question is now what will happen with the Parliament elections and Commission reshuffle coming up. The Commission will have to determine what actions might still be kicked off under the current Commission, and what exact proposal it will want to make at what time.
In any event, more and more developments seem to be converging that will likely lead to another revisiting of the MDR in the short term. And this will go beyond deadline amendments as nobody seems to want to amend the deadlines further.
For me personally a number of things need amending:
The EU system needs centralization of governance because the current decentralised approach does not work. There is too much difference between the way member states apply the MDR and IVDR and how they instruct notified bodies to apply these (as I notice in practice each day – try and obtain an article 59 MDR derogation for the same device in a number of member states, the diversity of approach and results are ‘interesting’).
Notified bodies can improve a lot in good administrative practice (although there are scattered initiatives to improve underway), while they are wielding delegated state power of control over market access. I notice in practice that member states control them rather poorly on this point and notified bodies are not able to recognise and correct their (procedural) mistakes quickly, resulting in devastating consequences for the manufacturer concerned. Let’s not forget that good administrative practice in exercise of government power is an EU constitutional right – we should expect the same level of diligence from notified bodies procedurally as we expect from authorities. Finally, there is often no meaningful appeal to a decision of a notified body after internal appeal at the notified body. It is often unclear in national law and not addressed at MDR/IVDR level if a court is competent to review a notified body decision. Legal review of exercise of state power is also an EU fundamental right. Yet, the MDR only provides for an explicit appeal pathway in case of a classification decision.
The approval system should be (much) more supportive of innovation and specific groups of devices (such as orphan devices). In other jurisdictions with which the Union is in regulatory competition special procedures exist for such devices, so this not be a question for the Union. Manufacturers (even EU ones) with the most innovative devices are more and more abandoning the Union as first jurisdiction of launch because the system is too slow, too costly and too unpredictable.
There is too much repeating bureaucracy under the MDR and IVDR. Especially the 5 years recertification cycle needs revisiting in view of the much increased PMS obligations under the MDR and IVDR. If periodic re-approval is not needed for medicines, why should it be needed for devices?
Much more attention is needed to the way horizontal legislation dovetails with the MDR and IVDR, especially where it comes to design changes that may need to be implemented for legacy devices as a result (e.g. Batteries Regulation, AI Regulation). Such changes are not automatically recognised as non-significant changes mind you and may therefore invalidate a legacy device certificate. More in general the regulatory lasagna created by stacking several layers of horizontal regulation on vertical regulation does not help for compliance. More in general double CE marking (as imposed by the AI Regulation for example) is just a bad idea. I understand that the MDCG and the AI Office under the soon to enter into force AI Regulation will do their best to synch policy and provide coherent guidance. But this should not be needed from a lawmaking perspective. It is infinitively unproductive to make law that is prohibitively complex to comply with (more about the AI Regulation on this blog in this respect when it enters into force).
Medical devices policy makers and market surveillance should be properly resourced, both on EU and national level. For a reason that entirely keep escaping me the level of resources devoted to policy and market surveillance in medicines is much much better while healthcare simply cannot function without medical devices and IVDs.
This was my personal wish list, and many other wish lists are circulating. Things are moving and positions converging. Now it’s time to fix the MDR and IVDR.
Happy birthday MDR and IVDR – I’m curious what the next one looks like!
In any event the new third edition of The Enriched MDR and IVDR will have been published by then, one of the reasons that this blog has received less attention from me than usual. Many people have told me that they miss it, so I will do my best to post more often again.
Some background: in the Netherlands we like to use taxes as a means to organise society by providing (dis)incentives through taxes. This is why we now have a tax system that is so complex that nobody understands it anymore and the tax service cannot even implement it reliably (this not made up or a personal opinion by the way). Also, for many of the tax (dis)incentives it is absolutely unclear if they achieve the intended effect because our government hates to do impact assessments for things that look nice politically.
Background
So what happened in this case? In the Netherlands we have two VAT (turnover tax) brackets: high (21%) and low (9%). This is great for policy by politicians, because you can move products and services around between these brackets. You can subsidize certain professions or products to look like you are really helping people, which Dutch politicians liek to do, especially with elections in sight.
For historical reasons medicines are in the low VAT bracket and medical devices are in the high VAT bracket. Since the Netherlands is a state of law, we have legal principles underlying taxes, such as the principle of fiscal neutrality (which is also an EU tax principle by the way). That means (in short, because the application is actually complicated legal voodoo that you can use in anyway as is opportune for tax collection as we will see in this case as well, as I’ve blogged about before on this blog in relation to customs law characterisation of products) that products that serve the same purpose for a consumer should be taxed in the same way, because that would be fair and non-arbitrary.
A medical devices company with a substance based device that does the same as some medicines decided to challenge the high VAT rate applied to its products based on violation of the principle of tax neutrality and then ran into what I can only qualify as an impressive exercise in regulatory bias based on prejudices about medical devices regulation, without empirical basis.
No empirical basis? It is actually confirmed in the judgement where it says that the lower courts could suffice by conceiving an abstract idea of how the consumer chooses between interchangable medicines and medical devices that are indicated for the same treatment rather than check how consumers really think by means of market research.
I must concede here that the European Court’s case law provides that a national court is not obliged to order market research under all circumstances when having to decide how the decision pattern of the average consumer works in a given factual context. However, the European Court, wise as it is, also holds that it may be very prudent to do market research to support a national court decision on this point. To which I will add: and it would be nice if the court also takes the trouble to be properly briefed about how medical devices regulation actually works. Both of these things did not happen in this case and then the results can be case law that does not look convincing at all and gives a strong whiff of regulatory bias between the medicines and medical devices regulatory frameworks.
More detail: the lower court landed on the ruling that the products concerned (over the counter medicines and over the counter devices for the same therapeutic indication) were not similar for consumers because:
the regulatory regime is different; and
the use of the product is different.
Let’s how the Supreme Court paraphrases this (this is my unoffical translation from the judgment in Dutch):
“3.4 The Court took as its starting point that the principle of fiscal neutrality applicable to the levying of turnover tax precludes the different treatment for turnover tax purposes of supplies of goods that are similar from the point of view of the average consumer. Artificial distinctions based on insignificant differences are to be avoided. In the Court’s view, the non-prescription registered medicines to which the interested party compares are not similar to the S products. Not only do the legal framework and legal regime under which each of these groups of products falls differ, but also their use is not similar. Here, the Court took into account that suppliers of registered medicines, including those that may be supplied to consumers without a prescription from a general practitioner or medical specialist, have to comply with different and more stringent requirements and undergo a more extensive procedure in terms of market authorisation, quality, efficacy and risks of those products and informing consumers about them, than that which the interested party has to comply with as a supplier of the products. The supervision of (non-prescription) medicines is also stricter. Monitoring the quality of medicines on the market is an ongoing process. In contrast, the Health and Youth Inspectorate checks only by means of a random sample whether medical devices indeed fall under the low risk class claimed by the manufacturer and meet the other requirements, the Court said.
3.5 Although the Court of Appeal considers it plausible that the S-products and the non-prescription medicines referred to by the interested party have similar properties as regards the treatment of the skin conditions referred to above in 2.1, in the Court of Appeal’s opinion, the interested party has not made it plausible that the differences described above in 3.4 do not play a role for the average consumer. The Court of Appeal considers it plausible that for the average consumer the quality and control guarantees surrounding registered medicines may be a decisive factor when making a choice between a registered medicine and (one of) the S-products. For the average consumer, the registration of a product as a medicinal product constitutes an important indication of the reliability of its efficacy and safety, which is underlined by the legally required comprehensive package leaflet containing relevant information on the efficacy, side effects and any other risks associated with the use of the medicinal product, the Court said. Since the S-products do not meet the requirements set out in the Medicines Act, nor are those products presented to customers as registered medicines, the Court does not consider it plausible that the S-products are nevertheless interchangeable with the non-prescription medicines referred to by the interested party in the eyes of the average consumer. The fact that the S-products must comply with the requirements of Directive 93/42/EEC does not make them medicinal products within the meaning of the Medicines Act, the Court continued.”
X / de STAATSSECRETARIS VAN FINANCIËN, Supreme Court 8 September 2023, ECLI:NL:HR:2023:1124
Mind you, this reasoning has not been based on factual research about what consumers actually think. This was conceived by the lower court in abstracto without the court thinking that it might be good to back this up with some facts. The Supreme Court upheld the lower court’s judgment on all points.
What does this mean? Apparently according to the Supreme Court:
Consumers (apparently) attach decisive importance to the regulatory supervision of similar products, and will choose the one regulated more ‘extensively’
Medicines in general but also over the counter medicines are subject to different and more stringent requirements and undergo a more extensive procedure in terms of market authorisation, quality, efficacy and risks of those products and informing consumers about them
For the average consumer, the registration of a product as a medicinal product constitutes an important indication of the reliability of its efficacy and safety, which is underlined by the legally required comprehensive package leaflet containing relevant information on the efficacy, side effects and any other risks associated with the use of the medicinal product
Complying with medical devices law does not make your product a medicinal product so it’s less attractive to consumers and therefore not interchangeable for tax purposes and can therefore be taxed differently.
Let’s unpack this.
Do consumers attach importance to the regulatory regime?
I do not believe for one single second that consumers attach importance to the regulatory framework under which a product is regulated. I really don’t. Rather, I think that consumers attach importance to the products being safe and effictive, regardless of the regulatory framework. This is the basis of EU product law for healthcare products: ensure a high level of public health and a high level of consumer protection. Medical devices regulation really is not intended by the EU legislator to do any concessions on these points compared to other legislation for other products. Rather, different products are subjec to different regulatory approaches, each proportionate and suited to the products in scope.
If it were true that the regulatory approval system of any product would decisively matter to consumers, this would lead to some truly bizarre situations. For example: consumers would always choose birth control pills (medicine) over condoms (medical device) for anti-conception purposes because the pill is a medicine and therefore obviously superior. Can you see how absurd that would be? I can tell you that I’m really glad that my own young adult children think about these things differently than the courts. More in general (if this theory of regulatory approval regime is a decisive factor in choosing) consumers would prefer to travel by airplane over travel by train, because airplane type approval is more ‘extensive’ regulation than train type approval and of course: consumers are deemed aware of this. People in the Netherlands would abandon their bicycles en masse in favor of cars because motor vehicles are subject to the stricter regime of type approval whereas bicycles only fall under the rather low end general product safety requirements (plus a batteries and EMC/LVD top up for e-bikes, which should have people preferring e-bikes over normal bikes because they are regulated more strictly).
If the court would have taken the trouble to do a descente (technical procedural law term meaning that the court leaves the court building to go look at a real thing happening in real life) to the real world and visited a drug store (where they sell the products concerned in this case) instead of dreaming up this theory in the privacy of its chambers, ask yourself if it would be possible that the court would have witnessed the following conversion:
[enter customer while court members browsing products are trying to look unsuspicious in various places in the drug store]
Customer: “Good morning, do you have something for [skin problem]?”
Sales person: “Good morning sir, we sure do. Would you come with me please?”
They walk to a shelf where a lot of colorful boxes with lots of letters on them are stacked under a big sign on the ceiling saying “SKIN”.
Sales person takes two boxes from the shelf: “Here sir, we have product [A] and product [B].”
These two products happen to be both creams, one a medical device and the other a medicine because they have a different mode of action.
Customer looks at the colorful boxes: “Which one do you recommend?”
Sales person: “Well, they both work for your skin problem. They have a bit of a neutral scent. Customers seem to be happy with either of them. But we sell most of these. [indicates medical device box]”
Customer: “In that case I want the medicine one.”
Sales person: “Oh?”
Customer: “Because the approval system is stricter and it has better post market follow up.”
Customer takes boxes from the sales person examines boxes by turning them in all directions.
Customer: “Yes, look, here. Here is the CE mark for the medical device product.”
[customer grimaces disapprovingly]
Customer continues: “And here is the RVG number for the medicinal product. So I’m taking that one. You can put the medical device back. Nobody wants that, with its substandard regulatory approval system. I’m surprised you even bother trying to sell this stuff. Nobody wants medical devices if they can get medicines for the same thing.”
Sales person: “Alright sir. Would you like me to give you more information about the medicinal product? Like about possible side effects?”
Consumer: “No thanks, I’ve got my medicinal product – that’s all I’m interested in. Nothing can top that and I’m sure these products are the best and that side effects for me are properly risk managed. I am of course going to read the patient leaflet from top to bottom. Can I pay please?”
Sounds absurd? Of course I’ve added some poetic license to show in this example dialogue how absurd the Supreme Court’s argument about assumed customer preference is, but essentially it reflects the argument 100%.
I hope you agree by now that this line of argumentation is not that realistic if not supported by facts about what consumers really think and what properties of products with similar intended use really matter to them. I am willing to bet a very good bottle of wine that the regulatory regime is utterly irrelevant to the average consumer. The average consumer expects something that is safe and effective, and will assume that any rules applied to any product publicly available will produce that outcome.
The most cynical point about this case is that the Appelate Court ruled that, when deciding whether product are similar for fiscal neutrality purposes, ‘artificial distinctions and insignificant differences are to be avoided’ (“Daarbij moeten kunstmatige onderscheiden op basis van onbeduidende verschillen worden vermeden.” – Supreme Court judgment section 3.4).
Misunderstandings
The judgment contains – in my modest opinion – some misunderstandings about medical devices law as it applies currently (or rather, already does since 26 May 2021) with the MDR. The Supreme Court and lower courts mention a number of determining characteristics that make medicines regulation apparently more attractive to consumers:
“more extensive procedure in terms of market authorisation, quality, efficacy and risks of those products and informing consumers about them, than that which the interested party has to comply with as a supplier of the products”
“The supervision of (non-prescription) medicines is also stricter. Monitoring the quality of medicines on the market is an ongoing process.”
“In contrast, the Health and Youth Inspectorate checks only by means of a random sample whether medical devices indeed fall under the low risk class claimed by the manufacturer and meet the other requirements.”
Let’s address these three points one by one.
More extensive procedure?
If you compare apples and oranges, a comparison never produces a relevant outcome. That’s basic logic. As I’ve shown with the examples above, the comparison between regulatory regimes for different products serves no purpose. It makes no sense to measure a product by a yardstick that doesn’t apply to it. A nuclear plant has a more extensive approval process than the solar panels on the roof of my house. Yet they serve the exact same purpose for me: produce electricity. And I am happy that each is controlled by a regulatory regime appropriate to it, ensuring that it is safe and effective for its purpose. But it does not mean that I favor nuclear generated electricity because the regulatory regime for nuclear plants is more extensive.
In the cases where borderline products are concerned (typically the category of substance based devices under rule 21 of Annex VIII MDR), it is important to note that under the MDR the conformity assessment procedure has become a lot more complex and now also includes an assessment of the quality of the substance by the medicinal products authorities, which leads to the interresting situation that with this the Supreme Court’s comparison argument is even less valid, because the same authortiy looks at substance quality of both groups of products (medicines and substance based devices). It means that if this case would be re-litigated for a substance based device under the MDR, the Supreme Court would need to come up with a new argument.
Stricter PMS and supervision?
Same point as previous, but worth to repeat verbatim: if you compare apples and oranges, a comparison never produces a relevant outcome. That’s basic logic. You learn this in basic math. But, tax is voodoo with different logic apparently. In tax law you can say that a fish is less evolved than a monkey because it doesn’t climb trees and that people therefore like monkeys better.
Apart from this, there is the underlying assumption that PMS and supervision of medical devices is so much more inferior that this would be (a) known the average consumer and (b) relevant to the average consumer and (c) relevant in the overall quality of supervision.
Since 26 May 2021 the MDR has added – for all devices in the market, including the legacy ones, and even the class I devices – the MDR PMS requirements which are very elaborate and apply to the entire life cycle of the device, even for class I self certified devices.
The Supreme Court would have done well to for example check with the competent authority for pharmacovilance and medical devices PMS and vigilance (IGJ) about what they think. If the IGJ would have been asked on the spot which one is better, I think that the IGJ would have said that both serve their respective purpose for the products in scope as well as they can.
Competent authority only performs sample checks?
This is just not true. Both under the MDD and MDR, and even for class I devices, the manufacturer has to monitor how the device is doing in the market by means of vigilance monitoring and report to the authorities any incidents that qualify as reportable. In case of any device above class I the device is (and was under the MDD too) subject to surveillance by the notified body that issued the CE certificate that is mandatory for classes IIa and up, as well as for sterile devices and devices with a measuring function (and under the MDR reusable surgical instruments, but these are usually not sold over the counter to consumers so not relevant in this picutre).
This means that the Supreme Court has either been misinformed on this point or misunderstood the argumentation that parties provided. In either case, all the more reason to revisit this.
Community loyalty?
The judgment is also, in my view, quite presumptuous about the comparative quality of (in both cases) European legislation. It suggests that medical devices are supervised ‘worse’ and that this is also obvious to consumers to the point that it determines their preference.
I would assume that the task of a Supreme Court is not to make value judgements about the comparative quality of different sets of EU legislation for different products, but rather decide on issues of law (what regime applies) and not of preference (what regime is better).
The respective products are monitored differently because they are very different products that work differently and are each subject to regulatory controls that the EU legislator has deemed effective and proportional for the products concerned.
In my opinion this presumptuous second guessing is at odds with the principle of Community loyalty of EU member states. The Supreme Court might have asked the EU Court if fundamentals of EU law even allow making this kind of distinction for the purpose of VAT law (which, also, is EU law by the way).
Anyways
As stated at the beginning of this post, I think that this case would have been more appropriately decided under Mandalorian Creed. The Supreme Court might get some inspiration from the Mandalorians, a humble warrior caste from the Star Wars universe that is low on value judgments because the Mandalorians know that knowledge is by definition empirical, i.e. fact based. Because this is the way.
As my examples show, the abstract argumentation used is spectacularly unhelpful in this case because it is not convincing, compares apples and oranges and looks arbitrary.
As much as everyone likes to pay taxes, me included, a credible application of the principle of neutrality in taxes does help for a good legal basis for the tax measure concerned. Making a hypothetical distinction between regulatory approval systems and attributing that to the average consumer without any factual backup does not serve that purpose of a solid legal basis. It sounds abritrary, which is not a lawful basis for imposing tax to begin with. We need a substantiation that at least sounds somewhat rational and is preferably tax based.
I hope that another company will have the guts and stamina to re-litigate this case with explicit reference to the MDR (because the present case only looked at the MDD) and the need to support this with some hard facts. That should lead to a different outcome, especially for devices that have gone through MDR conformity assessment. If that company needs someone for the devices and medicines argumentation, please count me in because the good part about mistakes in (case) law is that they can always be corrected. As the Mandalorians would say: this is the way.
Or in other words that I’ve asked on this blog before: can the maker repair what he makes? This blog will argue that he can and he should.
It still happens to me: people that say that the MDR or IVDR is ‘new’. In a way of course they are if you look at things on a cosmic timescale, but in objective terms the MDR or IVDR cannot be seen as new anymore – more as renewing because of the constant stream of MDCG (and to a less extent Commission) guidance to fill in the many gaps and the many amendments that have been adopted to keep the MDR and IVDR projects from derailing. Also, it could be seen as new in the sense of ‘naive’, because crucial elements needed to make the MDR and IVDR work properly have not been put into place, notably Eudamed.
But the MDR and IVDR are already so not new anymore. The Commission is already looking into the future to the date of 26 May 2027, on which it needs to deliver its report according to article 121 MDR and 111 IVDR to
“assess the application of [the MDR / IVDR ] and produce an evaluation report on the progress towards achievement of the objectives contained herein including an assessment of the resources required to implement this Regulation. Special attention shall be given to the traceability of medical devices through the storage, pursuant to [Article 27 MDR / 24 IVDR], of the UDI by economic operators, health institutions and health professionals”.
Article 121 MDR / 111 IVDR
Remember that the MDR and IVDR were first proposed on 26 September 2012 (11 years ago almost), entered into force on 26 May 2017 and are applicable since 26 May 2021 and 26 May 2022 respectively. This can hardly been seen as new legislation.
The Commission (DG SANTE) has now tasked EY to conduct a study that may provide part of the factual basis for the article 121 MDR report, the EY-coordinated “Study on Regulatory Governance and Innovation in the field of Medical Devices” conducted on behalf of the DG SANTE of the European Commission, for which I am honoured to function as an advisory group member.
Howhave the MDR and IVDR been doing?
With hindsight everything is clear and obvious of course. However, from my own experience and legal practice that gives me a statistically relevant view on the medical devices market I can mention a number of points:
The policy choice of not grandfathering devices and notified bodies, combined with an EU under-resourced process for processing notified body applications for designation under the regulations has caused most of the problems that are ongoing with the MDR and IVDR. That the designation process is still not up to speed is shown by the latest Commission figures that show out of a total of 62 applications for MDR designation since 26 November 2017 39 have been designated and out of a total of 22 IVDR applications since 26 November 2017 only 10 have been designated by 22 August 2023. These figures also show that the notified bodies still underway are mostly held up in the JAT review stage. This has also led to the by now notorious bottlenecks that have led to the MDR first having been delayed in becoming applicable and fat-going changes to the transitional regimes in the sense that the already complex legacy device situation became a lot more complicated. This added complexity is supposed to function as a pressure valve for the notified bodies but creates other problems because by now the transitional regime is so complicated that you need Commission Guidance (already in version 2) and Commission provided flowcharts to understand it, and needs to be explained to third countryauthorities who really don’t understand anymore.
The MDR and IVDR were built on the assumption that the data flowing through Eudamed would provide the backbone of the regulations. With more than eight years past entry into force of the regulations we are still not close to full functionality and mandatory application of Eudamed. What has arisen is a confusing patchwork of practices and policies by national competent authorities and notified bodies to utilise what parts of Eudamed are already online for use on a voluntary basis, and make that use mandatory in different ways, or diverge completely by setting up national databases and/or expanding existing systems.
The continuous adaption of MDCG guidance of which the authorities expect stakeholders to follow this without transition period and to the letter has made the MDR a moving target for notified bodies and economic operators. Also, implementing de facto binding rules by means of guidance is very much at odds with proper legislative procedure in a democratic society. The process of adoption of guidance has often been without due regard to stakeholder feedback and development of guidance intended with legal effect by non-lawyers (MDCG). This has led to guidance having been adopted that is ambiguous, sometimes manifestly wrong (PRRC – referring to EU instead of Union), created new obligations (MDCG 2021-27 on 2nd importer), perpetuated confusion caused by translation issues in other guidance (MDCG 2021-27 on placing on the market) or was adopted and applied regardless of its rejection of core principles by multiple member states (2022-5 on borderlines).
The MDR and IVDR have not solved a number of issues under the directives, specifically the problem that decisions with binding legal effect exercising delegated state authority (certification as a condition for market access) are taken without proper legal procedure and without proper legal review rights.
The costs and unpredictability of the route to MDR and IVDR compliance have caused many clients of mine to ‘rationalize’ their portfolios, i.e. decide that certain devices are not or not in the near future going to be on the market in the Union. This is being felt by health institutions, who bitterly complain about this. Data from April 2022 show that more than 50% of the medical devices companies are planning portfolio reductions, affecting 33% of these companies’ devices as planned for discontinuation. For IVDs 17% of today’s IVD total market will be discontinued, of which 50% is discontinued by small and medium sized enterprises (SMEs).
SMEs turn out to be impacted more by the MDR and IVDR than larger companies, although they represent 95% of the medical devices and IVD manufacturers in Europe. Discontinuation decisions taken by many SMEs largely are based on the expectation that the IVDR remediation cost will outweigh the product revenue. This happens on top of the devices that have already been discontinued since the entry into force of both regulations on 26 May 2017 and regardless of the additional legacy devices expected to be discontinued by the end of the grace periods for the MDR and IVDR in case their transition to the MDR or IVDR is unsuccessful.
Clients are dropping the customary Europe first strategy (see also the BCG findings last year), because Europe is being outcompeted by regulatory systems for large market that lead to a much quicker and less costly approval (also taking lifetime cost of compliance for devices). Especially manufacturers complex software devices with AI and very innovative devices for which there is limited clinical data available take the decision to go to other markets where they are met with a red carpet rather than a closed door or unpredictable conformity assessment obstacle course.
You could choose to think that if the measures taken to change the MDR and IVDR transitional regimes do their work we just need to power through this temporary difficult period and the situation will ‘normalise’ in the mid term (one of the assumptions of the Joint Implementation Plan for the MDR). This thinking is misguided in my view because the devices industry is one of long term planning and in that sense resembles a coral reef: whatever you destroy of scare away does not grow back quickly or return immediately. Another resemblance is the sensitivity to environmental conditions and human misunderstanding of this (raise temperature 2 degrees Celcius, how bad can it be?). By now most people do realise how bad it can be with coral reefs. It would be a shame if we would need to end up at that point with devices before we realise that the problem really needs solving. I have written on this blog years ago that we could be going down the ATMP regulation road with the MDR and IVDR (the EU regulation that killed the SME markt for tissue, cell and gene therapy by making market access overly complicated, unreliable and costly and I really hate to say ‘told you so’ but the data for MDR and IVDR is showing that exactly this development is going on and catching momentum. As MedTech Europe concludes: “MDR is currently a disincentive against launching medical device innovation in the EU.” This is absolutely not where we would like to be with medical devices policy for the Union.
Yes, the MDR and IVDR are a step up from the directives, but looking back I cannot personally say that I think that they have performed according to expectations. While they have been made as well as they could be made (yes, Bladerunner reference) they have not been implemented as well as they could be implemented.
But, we will see what the Commission concludes in 2027.
We should not forget that the functioning of the MDR and IVDR is not an abstract concept without consequences in the real world – don’t forget that we are all (potential) patients or users of devices. A malfunctioning MDR and IVDR impact innovation in medical devices and impact individual patient health: a treatment may not be available because the device is not available, which impact the quality of healthcare. There is a growing body of data collected by MedTech Europe that shows that innovation, patients and the quality of healthcare are suffering as a result of the sub-optimal functioning of the MDR and IVDR.
The BVMed and VDGH White paper on the Future Development of the MDR and IVDR
The question is if we can afford to wait until 2027 with starting a dialogue about how the MDR and IVDR have been performing, and whether they need any tweaks to make them work better, when the writing is on the wall already. Data collected and reported about the MDR and the IVDR by MedTech Europe published paint a pretty grim picture [link to reports], both as regards availability of devices in the Union in the near and mid-term future and as regards the innovation climate for the medical technology industry in the Union.
To make something stagnant move again, you sometimes have to cause some waves. BVMed and VDHG, the German industry associations for medical devices and IVDs, have just published white paper with the aim to a start discussion on how to make the MDR and IVDR can be made future-proof beyond the quick fixes and ‘delays’ by proposing potential options for the further development of the regulatory system for medical devices after the final transition from the Directives to MDR and IVDR and ensure their full implementation, in the short, mid and long term.
The white paper was developed, refined, commented on and finished by BVMed and VDHG in cooperation with their members over the course of a few months, during which I have spent an exhilarating time working on it in with the BVMed and VDGH team.
The white paper has gotten significant traction with other medical technology industry associations in other member states too, such as France, Spain, Italy, Spain, Austria, Switzerland and the UK.
I encourage all interested to read the white paper (published today and available here at BVMed and here at VDGH), and I know that it has already been received with interest by the Commission, member states, notified bodies and other stakeholders. The following is not a summary of the white paper, but rather my own personal perspective on its context. This blog therefore does not necessarily reflect BVMed’s or VDGH’s position, but is rather my very personal view on the white paper. The below summary is therefore also a very high level summary, the white paper itself is much richer with details.
The white paper consists of five pillars and is drafted in the ‘problem – context – solution’-model for each subject within a pillar:
Proposals to amend the regulations with missing elements currently missing, such as a procedure for orphan devices;
Proposals to increase efficiency of the system and implement principles of good administration;
Reformation of the standard five-year certification cycle;
International cooperation and reliance; and
Centralisation of responsibility.
Supplement regulations
The MDR and the IVDR are intended to improve healthcare for all patients, yet they do not do justice to all patients because they do not contain regimes for devices for specific groups of patients with very specific conditions, such as rare diseases or a specific age group (pediatric devices). They also do not contain an orphan devices regime. Other jurisdictions with a developed regulatory regime for devices have such procedures, such as the US, China, Japan and Brazil. The lack of an effective regime under the MDR has been observed by clinicians in the CORE-MD project as well, and has been identified as a missed opportunity in a peer reviewed publication authored by several well-known paediatric specialists and a civil servant from the devices unit at the Commission.
Another missing element in the MDR is the option of fast tracking of assessment of specific devices, such as is possible under the highly successful FDA Breakthrough Devices program, which gives priority to review for innovative devices that enable a significant improvement in medical state of art. Other jurisdictions with evolved regulatory systems have similar pathways. The consequence is that in this globalised economy other regulatory systems are outcompeting the EU, which does not only not have similar procedures but also has the problem that the approval procedures it has has become unpredictable in terms of cost and duration. As a result an increasing number of European and other companies is abandoning the ‘Europe first’ strategy for market access that has served the EU very well for decades. The white paper recommends adopting a similar procedure for the Union.
Increase efficiency and principles of good administration
The white paper makes a number of recommendations for improving efficiency of the regulatory approval system, which may be seen as a next step to flank the MDCG 2022-14 position paper measures, of which the effect unfortunately still is not really felt in the system because of the stunted roll-out of these no- legislative measures by the MDCG. As I have explained before on this blog, many of the points in the position paper are fully under control of the MDCG and the member states, or the MDCG is not part of a quick solution because procedures proposed by notified bodies in response to the position paper (such as a harmonised structured dialogue procedure) get held up at the MDCG. In that blog post I have referenced the Titanic and the member states as orchestra on the Titanic, and this still does not seem to have changed with the ponderous and unhurried pace at which the MDCG implements the actions in the position paper.
The proposals made in the white paper are intended to make the implementation and application of the rules more predictable, level the playing field for access to notified bodies and manage the overlap between national legislation and EU level rules better.
A long time point of mine is the implementation of principles of good administration, which should be inherent to any regulatory system as a matter of checks and balances in a democratic society and protection of fundamental rights of citizens. These also overlap largely with WTO recommended good regulatory practices for medical products, which include under this heading ‘legality’ as key elements:
The regulatory framework should provide the necessary authority, scope and flexibility to safeguard and promote health.
Delegation of power and responsibilities to various levels of the regulatory system should be clear and explicit.
Systems should be in place to ensure that regulatory decisions and sanctions can be reviewed.
The regulatory framework should clearly define the scope and lines of authority of the institutions that form the regulatory system to ensure its integrity.
The regulatory authority must be held accountable for its actions and decisions to the public, those regulated and the government within a legal framework.
Yet, the MDR and IVDR are seriously lacking in some of these respects and should in my view take a large step to evolve as a serious regulatory system, if only for the reason that the lack of appeal and legal review options is at odds with the EU’s own principles of fundamental rights, as well as with the European Convention of Human Rights to which the EU member states are signatories. These principles require that where state authority affect the rights and obligations of citizens is exercised (you get or are denied a certificate entitling you to market access for your device) this authority must be subject to procedural and substantive controls for exercise of state authority, which it currently is not. The white paper proposes a number of solutions to help the MDR and IVDR evolve to more mature regulation compliant with fundamental rights.
Certification cycle
The cornerstone of the MDR and IVDR is the conformity assessment leading to a CE mark. Where notified bodies are needed for the conformity assessment the manufacturer can only declare conformity based on a certificate issued by the notified body. Currently these certificates have a five year validity, which means that – depending on the life cycle of a device – a device will undergo repeated re-certifcation. This is somewhat of an anomaly internationally in the regulation of medical products. The international standard for medicines and medical devices is initial regulatory approval followed by strict PMS over the life time of the device. The MDR and IVDR have implemented a system in which all of this happens (especially world class PMS, which is also a significant investment in terms of time and resources) but in addition the market approval is revisited every five years, adding massively to cost of compliance but also to administration required to process these repeat certifications of products with a spotless PMS record. For the authorities this is fine, as supervision is outsourced to notified bodies this way, but for industry this leads to growing problems – especially for devices that are not huge blockbusters. Under normal circumstances re-certification could be OK, but we are faced with capacity restrictions for years to come as a result of the massive amount of legacy devices that still need to be assessed for MDR and IVDR certificates.
These issues with the certification cycle and the costs of approval mentioned above come together in an example described in a recent peer reviewed publication of certain paediatric atrioseptomy catheters for which cost of regulatory assessment in Europe is €135 844 every 5 years compared to €3030 for the lifetime market access in the USA].
For these reasons the white paper proposes to rely more on the increased PMS controls and their surveillance by notified bodies under the MDR and IVDR rather than stick to the current certification cycle, which imposes a significant burden on the system in terms of costs and time. Such a cycle would be justified in other sectors to which CE marking applies because these regulations invariably are not subject to the same intense notified body surveilled PMS and PMCF/PMPF, but rather rely on market surveillance by competent authorities.
International cooperation and reliance
Since most devices are identical across the globe, international cooperation and reliance make a lot of sense. The IMDRF (and its predecessor GHTF) plays an important role in this respect. However, there is much more that the EU can do in terms of furthering recognition- and reliance practices and to promote international convergence of Union regulation. The white paper proposes a number of things, such as countering regulatory fragmentation by exploring revival of the existing EU—US mutual recognition agreement for medical devices (if only for the PMS and vigilance data exchange part) and exploring MRAs with the UK and Switzerland.
The white paper identifies a number of other areas where the EU can step up efforts, such as in serious EU MDSAP participation and recognizing MSDAP audit reports (presently only recognized indirectly, via notified body review).
Centralisation of responsibility
I have joked on occasion that the member states can sometimes be likened to the runners in the famous Monty Python sketch of the 100 meters for people without sense of direction, each runner running off in a different direction at the starting gun. Yet, this is not dissimilar to how the member states operate in the MDCG as a result of the decentralized responsibility that is inherent in the system.
An important example is member states explicitly dissenting with the core principles of important MDCG guidance (such as the definition of the concept of pharmacological mode of action in MDCG 2022-5, one of the most important principles for borderline qualifications – Italy and Germany explicitly distanced themselves, stating in no uncertain terms that
“The vague definitions do not support effective and aligned implementation of the legislation. Uncertainties among manufacturers, notified bodies and authorities should be avoided. This Guidance does not provide a common understanding of how the MDR should be applied in practice aiming at an effective and harmonised implementation of the legislation.” (Germany)
“The mode of action to qualify a substance as a medical device or a medicinal product is not sufficiently clear. In particular, the amended definition of “pharmacological means” is insufficient to clarify the issue. Although the introduction of the concept “typically at a molecular level” can help, on the other hand it’s still not enough to a clear application. Moreover the conclusions reported in the guidance in relation to devices incorporating, as an integral part a substance which, if used separately, would/may/can be considered a medicinal product, are controversial causing confusion in the application of the rule. These uncertainties do not help in a proper implementation of the legislation and should be avoided. The guidance does not provide a proper tool to an harmonized implementation of the MDR.” (Italy)
Does this sound like a harmonised approach to borderline devices? Not really. And this is only an example where the member states concerned did choose to publicly and explicitly dissent, rather than just do things differently at national level as is standard operating procedure. For example, during the COVID-19 epidemic certain member states (e.g. The Netherlands) allowed MDR audits to take place remotely, whereas others did not (Germany). There are other examples, like the application of the article 97 MDR / article 92 IVDR exemption for formal non-compliance.
The problem with the decentralized nature of the devices regulatory system in the Union is that nobody seems to feel completely responsible because nobody is. Member states typically ‘wait for Brussels’ when this is opportune, but will at the same time not hesitate to take measures that frustrate matters that Brussels does take up enormously, such as setting up national databases for devices and registration of economic operators where the Commission has asked them not to do this or restricting notified bodies in remote audits where the Commission says this is possible.
Establishing a central accountable managing structure for medical devices would have important advantages over the current system. It would lead to a scenario where good administration is applied to decisions concerning certificate grant and certification status, just like with medicinal products and as is actually required under the EU Charter of Human Rights and the European Convention on Human Rights (ECHR).
How further?
I am also specialised in EU pharmaceutical law, which gives me a unique perspective to compare the legal systems for medicines and medical devices. Although also the EU medicinal products regulatory system has its own issues (which is why it is radically revised at the moment to fix these by the way) it is much better developed in the field of legality aspects as referred to in the WTO recommended good regulatory practices for medical products. I often invite people to do the ‘what if this happened in medicines?’ thought experiment, which I have designed especially for politicians and authorities who often do not seem to realise the crucial role of medical technology in healthcare. I notice that especially politicians and civil servants in the ministries tend to see devices policy as something abstract that is outsourced to Europe and the private sector and can be managed on a national level with basically zero resources and low sense of urgency. The experiment confronts people with the harsh reality of regulatory karma: suboptimal rules and suboptimal policy affect everything downstream negatively, and forces one to answer the question if that leads to acceptable outcomes. This thought experiment is quite simple: for every issue with devices regulation and policy ask the question: ‘would we accept this in medicines regulation and policy’? After that first question ask the follow-up question: ‘so why is this acceptable for devices then?’ For example here is a simple one: would we accept for medicines marketing authorisations that there is no fixed duration for an approval procedure or that there is no legal recourse against a decision to decline a marketing authorisation? Of course we don’t accept that. So why do we accept it for devices? You tell me! I’ve been saying from the inception of the MDR and IVDR that this was a missed opportunity.
This experiment is useful for national politicians that often do not seem to realize to what extent they can make a positive difference in Brussels, by supporting harmonization and ensuring that the resources strapped structures function. They can make a positive difference in the MDCG, by making it actually work and to require that makes work of implementing its position papers. The slow implementing of MDCG 2022-14 is a case in point. We are still waiting for quite a number of things to happen that are completely under MDCG (structured dialogues anyone?) or individual member states’ control (they just need to make their own medicines agencies do the work needed).
In any event, whether or not we would accept something for medical devices that we would not accept for medicines, it’s important that the MDR and the IVDR start to function and deliver on their promise. Hopefully I’ll make a contribution to this with my work on the proposals in the BVMed and VDCG white paper and my work in the EY study for the Commission, because Europe deserves world class medical technology regulation. Some things need to be fixed, other things can be improved about the MDR and the IVDR and in my view we should not sit on our collective hands to to capitalise on the low hanging fruit changes.
It’s still not too late to work on this, and not everything needs to happen immediately or all at the same time, which is why the white paper contains a neat table with things to remedy in the short, medium and long term. There is a lot to choose from to improve different parts of the MDR and IVDR. We have a new Commission starting next year that can put its weight behind this. We have European Parliament members who have indicated that mere moving of deadlines is not enough to solve the issues with the MDR and the IVDR. Let’s hope we do not need to have see things get worse before things can get better.
It’s time to give Europe the medical technology regulations that the patients, users and innovators deserve and engage on this with improvements in the short, middle and long term.
Today is the day that the amendment, aka the ‘extension’, to the MDR enters into force because it was published in the EU’s Official Journal today, number L080. As you are reading this, the amendment now applies all throughout the Union as referenced in article 1 MDR and IVDR. Union as in not European Union, which is something different. This is one of the most often made mistakes in relation to the application of the MDR and IVDR: people (among which even the MDCG in some cases, such in as MDCG 2019-7 regarding the PRRC) referring to the geographic scope of application of the MDR and IVDR as EU, and completely ignoring that this is not even what the MDR and IVDR say, what the EEA Agreement provides (it extends the scope of the EU internal market to Norway, Iceland and Liechtenstein) and what the EU’s Customs Union with Turkey provides (extends the MDR and IVDR to Turkey). Anyway, fortunately this MDCG PRRC document is up for revision in Q2 2023. Let’s hope the good members of the MDCG address this in the future, because if I were the Turks, Icelanders, Liechtensteiners and Norwegians I would not be happy with structurally being mistakenly kept out of the Union for the MDR and IVDR, even by the MDCG.
Asking about the MDR or IVDR ’s geographic scope is a good test to determine if regulatory people really understand the subject matter. Because if you think it’s limited to the EU only, you are missing countries where the MDR and IVDR apply, and some pretty major ones at that (like Turkey). If you want to know also in exactly which overseas territories of these Union member states or exotic corners of Europe like Svalbard (also known as Spitsbergen) or the Holy See the MDR and IVDR apply and do not apply, check out the 2nd edition of my book, The Enriched MDR and IVDR. But Erik, you’re always such a nitpicker you might retort. Well, here’s a thought experiment: if you’re a US company (who often get this Union thing wrong), would you hire someone for US work that keeps insisting that FDA law does not apply in, say, the state of Washington? Or California? Or Hawaii?
But I digress on technicalities. You want to know about the amendment of course!
Let’s not forget that the amendment does not only concern the MDR, but also the IVDR, as it removes the sell-off periods for each of the IVDR’s grace periods. More about that below under Sell-off periods.
How does the amendment work? Anything new?
Well, it works exactly as I’ve already described in a previous blog post, since the text has not been changed at all during the legislative process. So it’s exactly the same as proposed on 6 January last. I hope you used that time well by preparing rather than waiting if something might still change because in the latter case you’ve been wasting precious time.
Still, here is a summary:
(1) Extension of the MDR transition period until 31 December 2027 and until and 31 December 2028 depending on the device’s risk class to be determined in accordance with the MDR classification rules. The extension is subject to several conditions to ensure that only safe devices, for which the manufacturer has submitted an application for MDR conformity assessment by 26 May 2024 at the latest, will benefit from the extended transition period.
(2) Extension of certificates’ validity, provided the conditions for the extension of the transition period are met. Also certificates that have already expired after 26 May 2021 may be considered to be valid if additional conditions are met.
(3) Transfer of appropriate surveillance to MDR notified bodies by 26 September 2024 at the latest.
(4) Introduction of a temporary derogation until 26 May 2026 from requirement for quality management system certificate for class III implantable custom-made devices, subject to conditions.
(5) Removal of the ‘sell-off’ date in MDR and IVDR, allowing devices that have been placed on the market before or during the transition periods and which are still in the supply chain to be further made available without time limitation.
If you have a legacy device that is eligible under the criteria of Article 120 (2) MDR as amended, it will have either been extended automatically or relived automatically today. Automatically, magically! Because that’s what legislation can do. No need for formal confirmation needed. Clarification probably – so read on. And maybe check the flowchart I posted earlier:
For importers and distributors it is important to realise that the amendment changes the concept of ‘legacy device’ dramatically into a device that meets new article 120 (2) and (3a) – (3e) MDR. If they have procedures in their QMS that define the concept of legacy device so they know what it is (how else could they otherwise see if the device is compliant?) they should amend these procedures immediately as the new definition has entered into force today. This definition is different from the one in MDCG 2021-25, mind you. As of today this MDCG guidance is outdated on this point, but it is not yet slated as under revision by the MDCG although it totally should be now because the core definition is outdated. That should definitely have had some priority with the MDCG, given the enormous role legacy devices will be playing in the Union for a long time now.
On the other hand, for importers and distributors of IVDs this is not relevant, as MDCG 2021-25 does not apply to the IVDR, so there is no formal IVDR legacy device concept (yet), which seems rather inconsistent since the IVDR has been applicable for almost a year.
How will I know?
How can I show to others that my certificate is actually valid? While the operation of the extension of or reliving of the duration of the certificates is automatic, that does not mean that you will automatically see this translated into a new or amended certificate. And the amendment does not provide for a mechanism for this. How you are going to prove to the rest of the world that your expired certificate is actually still valid is therefore somewhat of a mystery at this point. This should become clear in Q&A guidance that was scheduled to be published this week. But the good part is that the law is on your side, even if the guidance is slow or still lacking. There seems to be a project of the notified bodies underway for a model administrative annex to the certificate that says that the invalid certificate is nevertheless valid because the law says so. Also, you yourself should work on convincing rationale to explain to others how the certificate is nevertheless valid (or find yourself a ghost writer like me perhaps), e.g. to a competent authority that you have asked for a certificate of free sale, in case your notified body is slow, not ready with the template, or whatever.
Sounds somewhat counterintuitive if you consider what a certificate is supposed to do in the first place, but this is the consequence of the EU policy decision that directive certificates cannot be amended anymore after 26 May 2021, when the MDR became applicable and the AIMDD and MDD were repealed.
Other known unknowns
There are still other known unknown as well, such as what a substitute device is. Maybe these questions are also answered in the Q&A document that we have not seen yet. Maybe that document will even be published later today. In any event, watch this blog and my LinkedIn.
Sell-off periods
The sell-off periods in both the regulations are removed. This means that devices that are placed on the market in the Union (not the EU, but the Union – different things, as explained above) in time before the expiry of the certificate can be sold off for ever, which is actually a pretty long time (of course limited by expiry dates for sterility and such). That means that all economic operators with article 13 and 14 MDR obligations will need to be able to distinguish between MDR and legacy devices forever, as discussed above. Again, potentially a long time!
It’s a good thing that the MDCG is also revising MDCG 2021-27, in which the MDCG erroneously states that the transfer of a property right is a precondition for placing on the market, which is manifestly wrong if you look at the inconsistencies of the Blue Guide language versions and the internal inconsistencies in the Blue Guide that this interpretation creates. It would also be nice if the internally inconsistent language versions of the Blue Guide could also be amended on this point too.
It would take only a small corrigendum, how difficult is that. If the Commission could magically change the transitional regime of the MDR in 2019 with a just corrigendum, I’m pretty sure it’s not that hard to fix this error in non-binding guidance that is continuing to cause a lot of confusion in the market.
Everybody is part of the solution
I cannot stress enough that for the amendment to have the intended effect every stakeholder should be part of the solution: competent authorities, notified bodies and industry.
From what I’ve seen so far the first two groups are not chomping at the bit. This may not be a statistically relevant example but the first reaction of the Dutch Minister of Health on LinkedIn to the Council finishing the first reading was telling: manufacturers have to get a move on now to get MDR certified as soon as possible.
The Commission was a lot more diplomatic in its reaction, stating that everyone has a role to play; the Commission, the competent authorities, the notified bodies and industry are all responsible for making this work. In that sense I think the civil servants supporting the Dutch Minister really had not picked up what the amendment actually is about and this led to a stream of very angry comments to his post on LinkedIn. When the Dutch Minister was later asked by press whether the statement was intended to single out manufacturers the Minister’s spokesperson did give the right answer that all parties involved have a role to play. Still, if this is the knee-jerk reaction of competent authorities and governments in the Union, we are going to have a problem with the rollout as the competent authorities may not see themselves as part of the problem will not do their best to ensure an expedient roll-out of the 19 points of MDCG 2022-14, which itself by now dates back to September 2022. Yet, in practice do not yet see a lot happening in terms of action by competent authorities and notified bodies. I have seen notified bodies giving their customers the most technocratic of ‘computer says no’ answers when asked how the customer could best prepare for an amendment of which we knew exactly what it was going to say, and even stating to customers that it might be end 2023 before the amendment would be completely clear. Given the 26 May 2024 deadline for a regulatory filing under the MDR in the amendment this kind of behaviour is really not helpful at all.
In the mean time the Commission has delivered with two Commission delegated acts deferring the timing of the complete re-assessment of notified bodies, capacities of notified bodies and national designating authorities have been freed that can be used, in the former case, for the conduct of conformity assessment procedures and, in the latter case, for the designation of applicant conformity assessment bodies.
Manufacturers, for their part, should keep in mind that the amendment does not give them more time to get their MDR act together – it really does not. In all scenarios an MDR application must have been lodged by 26 May 2024 (even for the class III implantable custom made devices, in whose case it concerns an MDR QMS application) and manufacturers are well advised to definitely try to submit their MDR application not at the very last moment before 26 May 2024, because there will be chaos and mayhem just before that date. Just like every sane person can understand that you do not go Christmas shopping the day before Christmas for absolutely obvious reasons, the same applies to making your MDR submission May 2024: the system will be packed, log-jammed, overloaded – whatever you like to call it, and your application may not be considered timely lodged. And that would be a pity. So be a smart company and improve your chances by submitting earlier! Or join the big formalities lottery (also not clearly provided for in the amendment) to find out on 27 May 2024 about your 25 May 2024 submission being thrown out on a formality that you will not be able to fix anymore. That would not be good corporate risk management because having a valid CE mark only goes right to your core business continuity, so it is kind of important. If your management, or anyone in the company with responsibility in these matters, thinks that the year 2027 or 2028 is intended to give you as company more time and wants to act on it, consider these people a business risk to the company. The company should perhaps consider moving them to a position that is less risky to the company, like maybe mindful gardening in the company greens around the building or company barista. The only time you can buy under the amendment is the situation where your certificate is extended or relives, but you decide not to make an MDR application by 26 May 2024. In that scenario your certificate will be valid until 26 May 2024, but you would still need to meet the conditions for extension or reliving of the certificate in the first place (legacy cert not expired at date of entry into force of amendment (i.e. today), or article 59 derogation / article 97 exemption in place at date of entry into force of amendment (i.e. today).
There are still some knobs to turn to smooth out the biggest unexpected issues. It may be that the Commission and MDCG ease up a little on what will be deemed to be a formally lodged application by 26 May 2024 as required in the proposal. It may be that you are able to agree to a submission plan with the notified body that allows parts of the technical documentation to be provided later. But what that would look like needs to become clear and would (preferably) not differ from one notified body to the next.
The future
The Commission is already one step ahead, discussing the implementation of the amendment and the future of the EU’s medical devices regime, which is still in dire straits. According to an information note of the Commission for the 14 March EPSCO Council the MDR is way not in the safe zone and the amendment and MDCG 2022-14 roll-out will need everyone’s full attention and participation. In that sense I would urge competent authorities to closely monitor how their notified bodies are doing in terms of being part of the solution in that regard. On the other hand, the authorities themselves should not be part of the problem by keeping notified bodies in the dark about what additional flexibility they are now afforded.
Important about this Commission information note are the forward looking part and some conclusions from the past. The Commission considers it important to tackle a number of structural issues before the end of the extended transition periods:
issues related to orphan devices,
small manufacturers’ access to notified bodies,
length and costs of conformity assessment procedures, and
interplay between clinical trials for medicinal products and performance evaluation studies for in vitro diagnostics.
The Commission explicitly states that these issues have appeared within the current regulatory framework and have a negative impact on patient safety, public health and medical innovation, which is a big admission about how the Commission sees the success of the MDR so far, and what is causing the flaws in the MDR that have led to the MDR performing underwhelmingly. It also shows that the Commission does not seem to believe that the current actions on some of these points will actually do the trick.
For example, I personally have absolutely no confidence in the SME measures taken via the EU4health program (developing material and activities to support market operators, in particular SMEs, in meeting the requirements of the MDR and IVDR – too little, too late and not what is needed). What is needed is that SMEs are not turned down when they present themselves at a notified body. I’ve often made comparisons with medicines marketing authorization procedure. Would we accept there if an agency says: “we have no time for you because we have more interesting applicants that already take up all our time?”. Of course not. Yet, we are perfectly happy to have this situation exist and continue in medical devices. This is why more and more SMEs go US first these days: they have a reliable and predictable pathway at a well-organized agency that is happy to help (especially if you have breakthrough designation (which we don’t have in Europe either)). Even SMEs these days have options outside of Europe if their innovations are not appreciated here. And the worst is that their innovations have often been developed with EU or local financial support and subsidies or tax facilities – yes, that is how you waste capital and innovation. Congratulations. I see this happen with clients increasingly often and it frustrates me to no end.
The Commission will gather further evidence for the comprehensive evaluation of the MDR and IVDR due by May 2027 (Article 121 MDR and Article 111 IVDR). So let’s see how things go and let’s hope no time is wasted. As they say, never waste a good crisis, and now is a good time not to waste this one even further.
Short update on the MDR amendment proposal because quite a lot of people were expecting the European Parliament to take a final vote on the MDR amendment proposal today. A lot of them that watched the vote on the Parliament’s streaming services were surprised and disappointed that the vote seemed unclear: no vote on the text of the proposal? What was that?
To clarify what happened: today the Parliament voted on the request to treat the MDR proposal in the accelerated procedure, which was literally what it said in the Parliament’s agenda, so no surprise there if you know how this works. By the way, it’s an IVDR proposal too and not just an MDR party, as the IVDR sell-off period is proposed to be removed.
While it had been pre-discussed with the Commission that this would be put on the agenda and preferably adopted rapidly without issues, drama or amendments in the accelerated legislative procedure, rule 163 of the Parliament’s procedures still requires a vote on this. And that happened today.
The vote was unanimous and now the vote on the substance of the proposal is scheduled for Thursday 16 February. Amendments can (theoretically) still be proposed by the Parliament on Wednesday, but also on this point solid pre-discussion between the Commission and the ENVI committee will likely lead to a no amendment situation.
If you want to check out the proposal for inconsistencies between languages or in your own language (or in another of the many interesting ones we have in the EU), see here as it has been translated in all language versions (a requirement for adoption).
So please bear with the Parliament for just another two days until the vote on the proposal, and then some more days as the proposal will trickle through the publication process to the Official Journal.
And, as the name of the journal suggests, it’s not official until published in the Official Journal – and since the proposal indicates that the normal 20 days delay period after publication is foregone for this proposal – it will enter into force on the date of publication in the Official Journal and not before. There is no official timeline for that. For the last accelerated amendment to the MDR it took about a week between vote in the Parliament and publication in the Official Journal – Parliament vote was on 17 April 2020, and the amendment was published in the OJ on 24 April 2020 (one week later). So let’s hope they can be just as quick this time. I know that it will make a difference for certificates expiring already, so no time to waste!
In the mean time, the proposal leaves many questions unanswered, so if you have any: don’t hesitate to contact me because answering those questions is what I do best. And boy, did I answer a few about this proposal already. I can safely say that now (actually some time before already) is a good time to make some scenarios about how the proposed amendment will affect your devices business if you haven’t yet done so. Scenario anyone?
It did not turn out to be what I expected in all respects. First, it contained also an amendment to the IVDR: a removal of the sell-off period at the end of each of the stacked grace periods, which makes this proposal very relevant for the IVDR as well. Secondly but logically it also contain an amendment for custom made devices that I personally had not expected but with hindsight makes a lot of sense.
The proposal reminded me of the epic philosophical dialogue in the “I want more life father” scene in the movie Blade Runner, in which the soon to expire replicant Roy meets Tyrell, the person who invented him, and argues for “more life”, posing to Tyrell the existential question “Can the maker repair what he makes?”
Tyrell says he cannot change the facts of life [you have to transition to transition to the MDR sooner or later] and explains how difficult it is to change processes in a life form that is already underway [once a law has been adopted, changing it is always problematic and messy and sometimes may not fix the problems created already]. An intense argument about possible ways to do it follows, where Roy makes suggestions that are each falsified by Tyrell. Tyrell ends the discussion with his consolation “You were made as well as we could make you.”, which the EU legislator will no doubt think about the MDR. Let’s hope the MDR extension does not end like the Blade Runner scene, in which Tyrell does not survive the confrontation with his angry creation that does not accept his fate.
In the case of the MDR the extension comes at a price as we will see below. Age old wisdoms are that there is no such thing as a free extension and that you have to beware of people bearing gifts in situations where they might want something from you. In this case both of these old wisdoms apply. The MDCG has been warning for a long time that whatever is going to be done to help in terms of bridging and extensions is supposed to only benefit the manufacturers that have already taken steps to transition to the MDR. If your company has gambled and kick the can down the road, you will find that your options under this proposal are very limited, and intentionally so.
Let’s pick this proposal apart with the knowledge of now. The MDR part of the proposal completely upends article 120 sections (2), (3) and (4) MDR.
Article 120 (2) changes: validity of certificates
Article 120 (2) MDR is proposed to be changed to keep the valid (AI)MDD certificates valid or have them relive and be valid (in case of expired certificates) from the expiry date on the certificate for the period until the risk class based backstop date in the new article 120 (3b) (31 December 2027 or 2028).
Wait what? Expired certificates relive?! Yes, but only under conditions set out in the new article 120 (2) (a) and (b):
Either you have both signed an agreement with a notified body before the expiry of the certificate for the legacy device or a “a device intended to substitute that device” OR
You have a valid article 59 MDR derogation or a valid article 97 MDR exemption (either of which apparently does not have to be in place at the expiry date of the certificate, which makes sense).
An important question is what the concept of “a device intended to substitute that device” means, because this is a gating item both for the notified body and for the manufacturer. This concept is not clarified anywhere in the recitals or the explanation to the proposal, yet is a crucial concept for application of the amended transitional regime. For example: would this device need to be equivalent to the legacy device it is intended to replace? And is that then evaluated by reference to the criteria for equivalence under the MDR? Or can it be a device that has a broader intended purpose? Nobody knows and this concept will need Commission or MDCG clarification. And we all know what that means: this will not arrive soon.
The fact that this clause extends the validity of existing and valid legacy device certificates by operation of law from the expiry date (even if that date is still in the future) but also – in exchange – makes the article 120 (3b) – (3d) conditions immediately applicable to the device (see conditions discussion below). So whether you like it or not: with a still valid certificate as a result of automatic application of article 120 (2) MDR you are shunted into the new regime – no choice. What does that mean for you?
Article 120 (3) changes: stacked risk based grace periods
Interestingly for a change the MDR proposal follows an earlier IVDR legislative amendment, implemented early 2022, which implemented stacked grace periods by risk class. The MDR now copies this mechanism, as I predicted as a likely option, but adds additional conditions for the use of the extended grace periods that are aimed to foreclose the extended grace periods to manufacturers that do not meet one of the article 120 (2) conditions for certificates to be valid beyond their expiry date:
Either you have both signed an agreement with a notified body before the expiry of the certificate for the legacy device or a “a device intended to substitute that device” OR
You have a valid article 59 MDR derogation or a valid article 97 MDR exemption (either of which apparently does not have to be in place at the expiry date, which makes sense).
Let’s look at the details of what changes in article 120 (3). “Due to the length of the provision, paragraph 3 is replaced by paragraphs 3a to 3g.”, says the explanatory memorandum.
Article 120 (3a) – derogation from Article 5 MDR
This means that when you meet the requirements of the proposal (device qualifies under article 120 (3b) or (3c) MDR and you meet the conditions under article 120 (3d) MDR you get to be exempted from the core requirement in the MDR: having a valid CE marking under the MDR.
120 (3b) – to suture or not to suture?
Article 120 (3b) provides for triage of devices that are already subject to an (AI)MDD certificate. Triage happens based on risk class under Annex VIII of the MDR (the provision does not explicitly state this by the way, but this is consistent with the way the corrigendum for the up-classified class I devices worked) and on the basis of a qualification question that will have pained many for requirements for Well Established Technology (WET) under article 18 (3) MDR (implant card), article 52 (4) (conformity assessment) and 61 (6) (b) MDR (clinical evaluation requirements): the sutures, staples, dental fillings, dental braces, tooth crowns, screws, wedges, plates, wires, pins, clips and connectors. The proposal’s explanatory text refers to them specifically as WET. This means that more complex devices with these names are likely not in scope of this defined group. In this regard the Team-NB Position Paper on a risk-based approach for medical devices exempted from an implant card and information to be supplied to the patient with an implanted device per Article 18.3 may also be relevant for qualification and for dental implants the Team NB position paper on Applicability of exemption rule to endosseous dental implants and dental implant abutments may be relevant.
See for triage logic the below summary flowchart. Note please that this flowchart does not describe the full process and all applicable conditions – it’s for triage only. And it is an improvement on the flowchart I initially shared via LinkedIn.
Triage flowchart for MDR proposal
I posted a slightly different version of the flowchart in on LinkedIn initially that excluded sutures, staples, dental fillings, dental braces, tooth crowns, screws, wedges, plates, wires, pins, clips and connectors from the 2027 period altogether because of the use of the comma before the word ‘except’ in article 120 (3b) (a) (“31 December 2027, for class III devices and for class IIb implantable devices, except “sutures, staples, dental fillings, dental braces, tooth crowns, screws, wedges, plates, wires, pins, clips and connectors”) and the explanatory memorandum clarification
“The transition period is extended from 26 May 2024 until 31 December 2027 for higher risk devices (class III and class IIb implantable devices except certain devices for which the MDR provides exemptions, given that these devices are considered to be based on well established technologies) and until 31 December 2028 for medium and lower risk devices (other class IIb devices and class IIa, class Im, Is and Ir devices).”
Explanatory memorandum proposal
Later we heard that the Commission had clarified in response to a question that qualifying sutures, staples, dental fillings, dental braces, tooth crowns, screws, wedges, plates, wires, pins, clips and connectors end up in the 2028 bucket. So I had to amend my initial flow chart to the above version. Don’t use the old one!
What I personally don’t find very logical is why the deadline logic departs from the 26 May deadlines as used everywhere else in the MDR and IVDR and instead uses 31 December 2027 and 2028. It’s nice that there is more time for transition of course, even if it is not logical. At least chances that people get in trouble with this are slim, because at worst a company finds out on 26 May that they had until 31 December.
Also here we have the discussion of what a “device intended to substitute that device” is (see above under article 120 (2) MDR).
120 (3c) – the up-classifieds had better hurry towards MDR
Article 120 (3c) deals with the class I up-classifieds, or in other words: the devices that do not need a notified body certificate under the MDD, but will need one under the MDR. These had gotten the corrigendum 2019 bonus of a declaration of conformity issued before 26 May 2021 that could be valid until end of the game period, provided that the article 120 (3) MDR requirements keep being met, such as no significant changes. This proved a lot more difficult than expected for especially software devices. These devices now get four and a half years extra time: until 31 December 2028! Whoohoo!
But this comes at a price: for these devices you do need to meet the requirements under article 120 (3d) MDR now, which still include no significant changes until that date and most importantly, some big things you need to do before 26 May 2024: have a full MDR QMS implemented (article 120 (3d)) and have a conformity assessment application underway at a notified body, with which you need a written agreement too by that date (article 120 (3d) MDR). That means that as manufacturer of an up-classified device you must have met these condition more than four (4!) years ahead of the end of your transition period. And if you don’t, you lose validity of your declaration of conformity by 26 May 2024 and you are done under the MDD and MDR.
So think about this a second (makes underwater scuba sign for “think about this/do not forget to”): you will likely not get to use up the full time until end of 2028 under the MDD (unless your conformity assent procedure takes four and half years, which is unlikely). So if you have a class I up-classified device you actually have no time to lose! You have less than one and half years (until 26 May 2024) to be ready for MDR conformity assessment – now that’s something else than sitting on your hands until 31 December 2028, right? Ergo, please do not make that mistake. Time is of the essence now.
120 (3d) – there is no such things as a free extension
There is no such thing as a free extension, and this one also comes with strings attached. These strings are set out in article 120 (3d) and – mind you – they also apply to class I up-classified devices as discussed above. Some of the requirements are already in the MDR (article 120 (3) MDR): the requirement of continued compliance with the (AI)MDD (article 120 (3d) (a) MDR) and no significant changes in design or intended purpose (article 120 (3d) (b) MDR, as clarified in MDCG 2020-3), which is no change from the current situation. The other three conditions in article 120 (3d), however, most certainly are because they are new (although you could debate this for article 120 (3d) (c), which is already part of the appropriate surveillance for the (AI)MDD certificate).
Let’s start with article 120 (3d) (c), which requires that your device does “not present an unacceptable risk to the health or safety of patients, users or other persons, or to other aspects of the protection of public health”. This is very much a market surveillance term (only found in the MDR in the market surveillance provisions article 93 to 97, meaning that the competent authorities do not want to get in trouble with the device concerned). But how are you going to determine that? It’s your device, (AI)MDD certificate valid, so how on earth could it pose an unacceptable risk? The whole idea about having a valid (AI)MDD certificate is that the devices presents acceptable risks only. According to the explanatory note:
“No systematic check of the device’s safety is required, as devices covered by a certificate issued under the Directives will be under ‘appropriate surveillance’ by the body that issued the certificate or a notified body designated under the MDR. Where, as part of their market surveillance activities, a competent authority finds that a device presents an unacceptable risk to the health or safety of patients, users or other persons, or to other aspects of the protection of public health, the transition period ceases to apply for that device.”
OK, so how will the notified body apply this then, because it is not a conformity standard subject to appropriate surveillance? It looks like this refers to the criterion in section 4.5 of MDCG 2022-4 Rev. 1 (“where the audit activities reveal a major non-conformity, which may present an unacceptable risk to the health or safety of patients, users or other persons”) but which still remains very unclear externally, but the notifying authorities will probably have instructed notified bodies on how to apply this. Would be nice if the rest of us would know too, right? Makes it so much easier to comply with requirements.
Article 120 (3d )(d) requires, according to the explanation to the proposal that
“no later than 26 May 2024, the manufacturer has put in place a quality management system (QMS) in accordance with Article 10(9) of the MDR. This condition aims to ensure that manufacturers gradually move towards full compliance with the MDR requirements. No specific attestation, i.e. no self-declaration nor verification of the appropriateness of the QMS by a notified body, is required at this stage. However, by submitting an application for conformity assessment to a notified body (see next condition), the manufacturer implicitly confirms that its QMS is in compliance with the MDR.”
Explanatory memorandum proposal
This condition is intended to make all manufacturers of legacy devices march in line as regards QMS as of 26 May 2024, and a step up to the conditions that were already in article 120 (3) MDR, which required certain QMS parts to be implemented for legacy devices. This is now changed to the whole QMS enchillada.
So, wouldn’t the requirement to also have a conformity assessment application underway by that date make a non-requirement out of this provision? Why is this needed if the condition under 120 (3d) (e) of a conformity assessment application for MDR lodged is sufficient? Good question. Because the problem with legal requirements is that you have to meet them and that would be firmer than an implicit confirmation.
So what could be the consequence? This would – I think – only have consequences where the manufacturer fails the QMS audit under MDR (because then he did not have a compliant QMS in place) and the consequence of not meeting the requirement would be so-called ex tunc invalidity of the certificate, in which case it turns out that the manufacturer never met the requirement, was non compliant on 26 May 2024 or the date on which he submitted the conformity assessment application, meaning that the certificate was invalid and the manufacturer has been placing non-compliant devices on the market, which is a market surveillance no-no, subject to competent authority fines, imposed recalls and so on.
Finally, as last condition article 120 (3d) (e) requires that no later than 26 May 2024, the manufacturer, or an authorised representative, has lodged a formal application in accordance with Section 4.3, first subparagraph, of Annex VII for conformity assessment in respect of a device referred to in paragraphs 3b and 3c of this Article or in respect of a device intended to substitute that device, and no later than 26 September 2024 the notified body and the manufacturer have signed a written agreement in accordance with Section 4.3, second subparagraph, of Annex VII. Note that this need to concern the legacy device or the “device intended to substitute that device” (discussion above under article 120 (2) MDR). Also note that this condition contains an additional condition compared to article 120 (2) (a): not only is a written agreement needed, but the conformity assessment application must be have been lodged.
Effectively this means that the validity of certificate (dealt with under article 120 (2) (a) MDR) is treated differently than placing on the markt / putting into service under that valid certificate (which is dealt with under article 120 (3d): ‘devices may be placed on the market or put into service until the dates referred to in paragraphs 3b and 3c of this Article only if the following conditions are met’). I am not sure why this choice was made. It does allow for the option to have a valid certificate (may be useful for ex-Union trade) but not be able to place devices on the market in the Union. It also means however that a manufacturer must lodge an application for conformity assessment before 26 May 2024 to be able to keep placing devices on the market or put them into service. The question is also here what ‘lodged a formal application’ means: must the manufacturer have made an application or does the application also have to be validated and accepted by the notified body? That latter element does not follow from the text nor from the application, so this may mean that this will be tested in practice with a lot of applications being made shortly before 26 May 2024.
As long as the certificate or declaration of conformity is valid (which is until 26 May 2024 at the latest) you would expect not to be affected by the conditions for continued validity under article 120 (3b), (3c) and (3d) and could sit out your certificate quietly until the expiry date. But this is not how the proposal works as discussed above. Article 120 (2) as amended extends these certificates by operation of law immediately upon entry into force of the proposal to either 31 December 2027 or 2028 without giving you an option. Article 120 (3d) (e) provides that you must have lodged a conformity assessment application with a notified body and have signed an agreement with the notified body in order to for the certificate or DoC to remain valid. As stated above, this means that you cannot wait, but have to immediately start to prepare and submit the best conformity assessment application at a notified body that will accept it. Manufacturers may see that while they meet the 26 May 2024 deadline, the notified body then has a long time to complete the conformity assessment (but the manufacturer is rewarded with a certificate that remains valid until 31 December 2027 or 2028), hopefully giving the notified body enough time to complete the assessment before the legal expiry of the prolonged validity.
Also here it is relevant what happens when the application is rejected: was the placing on the market and putting into service until that time retroactively unlawful (ex tunc application) or will it only be unlawful for the future (ex nunc application)? The proposal is silent on this point
120 (3e) – the old conditions of article 120 (3) MDR remain in place
The old conditions of article 120 (3) remain in place for the legacy devices (MDR post-market surveillance, market surveillance, vigilance, registration of economic operators and of devices) but this is really only relevant until 26 May 2024, because after that date the manufacturer is running a full article 10 (9) MDR QMS.
120 (3f) – notified body shuffle
Article 120 (3f) deals with the logistics of which notified body is responsible for surveillance of the certificate when it remains valid past its expiry date (this does not need to be an MDR designated notified body), how it works when the legacy devices is substituted by another device. The MDR notified body with which the agreement is signed pursuant to article 120 (3d) (e) (the one that needs to be in place for the legacy device or the substitute device) takes over surveillance of the notified body that surveilled the legacy or substitute device certificate if this notified body was not designated under the MDR.
120 (g) – custom made devices have the least transition time
Class III custom made implants (which require notified body intervention under the MDR pursuant to article 52 (8) MDR, so it’s kind of logical that these are also covered in this proposal.
What I don’t understand it why their deadline is 26 May 2026 and not 31 December 2026, and why they did not go in the class III implants category of 31 December 2027. Maybe the Commission thinks that the custom made devices have an easier pathway or something? This is not necessarily the case.
The same conditions as under article 120 (3d) (e) apply: having an agreement signed with a notified body by 26 September 2024 and lodging an application by 26 May 2024.
Article 120 (4) changes: the sell-off period removed
The changes to article 120 (4) are to remove the sell-off period completely. This has been the result of a successful lobby effort demonstrating that the sell-off period was simply too short because most devices take a long time to move through the supply chain slower than the legislator initially assumed. Also, the devices stuck in the supply chain that the 27 May 2025 hard stop would be lost to the Union market, which would also be a bad idea. In the words of the proposal:
“To prevent unnecessary disposal of safe medical devices and in vitro diagnostic medical devices that are still in the supply chain, thus adding to the imminent risk of shortages of devices, such further making available of devices should be unlimited in time.”
Recital 10 of the proposal
This means that there will be unlimited time for selling off of legacy devices that were placed on the market lawfully and that there will be a considerable period of time in which there will still be legacy devices on the market being sold off, and competing with MDR certified devices. Apart from the confusion that no doubt will ensue about the compliance status of legacy devices still being sold off to end users in 2030 (which is possible)m the question is how fair this is to the manufacturers that did invest in MDR transition and may face competition from these devices for a considerable time. And to patients, that may be treated with old legacy devices while more state of art ones are available as MDR CE marked devices. The whole idea behind the sell-off period was in itself not bad: that at a certain point in time there would only be devices on the market approved by MDR standards.
Housekeeping (article 122 and 123)
There is some technical housekeeping in article 1 (2) and (3) of the proposal, making changes to articles 122 (repeal of directives) and 123 (delayed entry into force of provisions) to account for the changes made to article 120 in the proposal.
IVDR changes: the sell-off period removed
For the IVDR the proposal contains a removal of the sell-off period. The background there is that the Commission has realized that the sell-off period is simply too short and will lead to devices being stuck in the supply chain at the end of the sell-off period. In the words of recital 10 of the proposal:
“To prevent unnecessary disposal of safe medical devices and in vitro diagnostic medical devices that are still in the supply chain, thus adding to the imminent risk of shortages of devices, such further making available of devices should be unlimited in time.”
Recital 10 proposal
I must say that I had not expected this. This may have been done for the same reasons as for MDR medical devices, but it also invokes the same issues as with MDR medical devices: there will be legacy devices on the market having gained access under ‘old’ standards’ that will be competing with IVDR standards assessed devices for a potentially looong time (if the devices have long or no expiry dates).
Relation to MDCG 2022-18 (article 97 exemptions)
If the proposal is adopted, the extension by operation of law of legacy devices will massively decrease the potential burden on the competent authorities to solve things by means of recourse to article 97 MDR, for which MDCG 2022-18 provided the blueprint.
The competent authorities’ role will be limited to dealing with the exceptional cases that do not fit in the proposal logic for one or the other reason, just the way they like it and is their normal modus operandi.
Relation to MDCG 2022-14 position paper
No proposal is an island. As I have observed in an interview with RAPS, we will also need the MDCG and member states’ full and unwavering commitment to roll-out of MDCG 2022-14 measures to create enough room for the notified bodies to live up to the challenge. I have been somewhat critical about the MDCG’s capacity to deliver, but I would like to remain enthusiastic and hope that, in the spirit of the ‘can the maker repair what he makes’ the MDCG will surprise us all positively.
And manufacturers must step up too. At the risk of sounding like a broken record: this is no time to sit on your hands people. As explained above, the first deadline hurdles for MDR QMS and a lodged application for conformity assessment at a notified body that you may still need to find and willing to work for you and sign a conformity assessment agreement with by 26 May 2024 are closer than you think. If your management thinks that anything less than full throttle is a good idea in any way for MDR transition, they are not fit for purpose. The proposal makes MDR transition a Chefsache as they say in German (‘a matter for management’), more than ever.
Adoption process
The adoption process follows the same procedure as the rushed MDR date of application extension in 2020: the accelerated co-decision procedure, which at the time was formally completed at lightning speed in less than a month. This proposal is far more complicated, so I expect the institutional actors to take a bit more time (also some parliamentarians announced that they are not going to be rushed like the last time). It is possible that there are still amendments to the text.
So pretty please with sugar on top: not legally trained consultants, please don’t say that this proposal is it, that it’s official, that it has been published in the Official Journal (which will not be yet until adoption) – don’t jump your guns, leave law to the lawyers and wait until the legislative procedure has run its course. Only then we will know what the adopted law will be and what rules need to be observed.
There is a consultation about the proposal from 11 to 18 January, which initially and apparently mistaken was put up for the normal consultation period running well into March, which was hastily corrected by the Commission. You can still put in comments to the proposal but don’t expect too much of them actually changing the proposal as the Commission may (or not) pass some of the comments to the Council or Parliament. If you want to influence things, go directly via parliamentarians working on this dossier or the member states in the Council.
At this moment I myself expect the proposal to be adopted and enter into force (foregoing the normal 20 days waiting period after publication in the Official Journal because of the rush) in March, likely the second half of March.
Balancing the MDR and the IVDR grace periods
Interestingly, if the proposal is adopted the IVDR will have a much more lenient and simpler grace period regime than the MDR – is that useful, is it fair? Both have risk class stratified grace periods and came from a single grace period. The IVDR however has almost no conditions for use of the grace period, the MDR has a lot and frankly complex ones.
Will we see similar conditions under the IVDR as under 120 (3d) when the grace periods for the IVDR do not suffice? This may well be the case, because as we’ve seen the MDR and IVDR keep influencing each other in solutions adopted to make the transitional regime work. I would encourage the IVDR manufacturers to make the best possible use of the availability of notified body capacity at the moment to avoid having to deal with a panic fuelled similar regime change for the IVDR in the future.
Can the maker repair what he makes?
As explained above, the proposal leaves a lot of open ends, such as what a substitute device is. Open ends are exactly not what we need at this time, especially because they will require MDCG guidance to explain and MDCG guidance is never fast or on a reliable timetable. Where possible these points should be fixed in the legislative process because otherwise we will be dependent on MDCG guidance for clarification, which will simply take too long.
A thing that worries us lawyers are matters of ex tunc invalidity of certificates or ex nunc invalidity in case of not meeting conditions for extension. This is not a trivial technicality and should be addressed at least in a recital in the proposal.
The good part is that at least some of the (big) notified bodies think that the proposal gives them enough time. This is very positive indeed. The question is whether this is true for all notified bodies, and what member states will do to make sure to enable maximum use of the MDCG 2022-14 position paper measures for the notified bodies and oversee notified bodies’ serious engagement on these points. At this point I see some of the smaller MDR notified bodies in serious disarray at the moment, at the expense of their poor clients who are caught in the middle without proper legal recourse and captive by the mess the notified body is making of things.
The original grace period under article 120 (3) MDR was already difficult to explain to foreign authorities in jurisdictions that attach importance to the CE mark and often misunderstood far and wide, leading to situations where foreign authorities flat out refused to accept anything else than a shiny new MDR certificate because that made sense to them. The new grace period will be even harder to explain to foreign authorities and to member states’ authorities issuing free sales certificates. The Commission and member states must make work of explaining this internationally to avoid creating Confusion Everywhere. The EU medical devices regulatory system has already lost too much of its international reputation, we don’t need this to be exacerbated. Also, it remains to be seen how foreign authorities will deal with the removal of the sell-off period, because these forever legacy devices can be sold on the Union market lawfully, which means they can be covered by a free sales certificate. This means that we will be explaining to foreign authorities how this works for a potentially long time.
Like I’ve said above: crucial to the proposal succeeding is pro-active rollout of MDCG 2022-14 and a functional safety net from MDCG 2022-18. This is completely in the hands of the MDCG and the member states who have the opportunity now more than ever to show that medical devices policy is a serious matter and be as much part of the solution as they can be.
But first: let’s see how the legislative procedure unfolds, and what the proposal looks like when it is adopted.
What to expect for the MDR and IVDR in 2023? Predictions are very hard, especially if they are about the future. That’s a paraphrase of a very solid Danish nugget of wisdom attributed to the physicist and chemist Nils Bohr. But let’s see what we can do based on some basic extrapolation of things currently hanging in the air that I will discuss below in this blog.
I know that I have not been very positive about the MDR in 2022. In fact I’ve said that we are in a process of Verelendung with this regulation at the moment in which things first need to get worse before they can get better. I think this was not exaggerated at the time and still may not be at this moment. I also think that the IVDR is an accident waiting to happen in much the same way as the MDR, because all the same mistakes are being made, and some additional ones.
But … something is slowly starting to be done – actions are being taken with the intention to fix these problems.
Commission proposal to amend MDR transitional regime
After the Commission’s very generally worded outlines of a potential proposal presented on the 9 December 2022 EPSCO meeting I was personally amazed by quite a number of consultants calling this ‘an official proposal’ and some stating that MDD certificates would be ‘extended’, for both of which there was absolutely no (legal) basis whatsoever. This is unfortunate because this regulatory gun jumping does not help to make things clearer and only creates confusion – it’s always better to be correct than to be first when it comes to these things I would think.
The outlines of the potential proposal still leave a lot of gaps, as I have discussed on this blog earlier. We will need to see if the Commission actually makes a proposal early January as announced at the 9 December EPSCO meeting. The Commission has said it will so it is likely, but we also expected the proposal way earlier (on 9 December 2022) and ended up disappointed – the Commission can always still postpone it. We have also seen the Commission moving the Eudamed deadlines again and again and postpone the necessary measures for Annex XVI devices for years. Then we will still need to see what this proposal will look like exactly. Will it also revive MDD certificates that have already expired and under what circumstances? Will it extend the My 2024 end of grace period back stop date? How will it relate to the Article 97 MDR ‘bridging solution’ set out in MDCG 2022-18 (discussed below)? This is important because Article 97 MDR is only needed where the law, the MDR, does not provide for a solution allowing the manufacturer to be compliant for the device concerned. For example, if a change to article 120 (2) MDR for example extends the duration of certificates for legacy devices (which is a possibility according to the Commission), then less Article 97 MDR applications will have to be made, which would free up valuable competent authority capacity.
After it has been made the proposal then needs to go through the EU legislative procedure during which it may still be amended, so I expect nothing definite before end of March 2023 (and that is if they really speed up the legislative procedure, which may not happen because some Parliamentarians have indicated that they want to give this proper consideration and will not be rushed like last time with the MDR date of application move from 26 May 2020 to 26 may 2021).
So hold your horses when you say that the MDR transition period will be extended and that there is an official proposal but please wait for the moment that we really know what this will look like before making specific claims about the future of the MDR transitional regime. Plan for notified bodies waiting with any definite steps until the legislative proposal is actually law (not before March 2023 likely).
There may be more in the proposal that was not discussed yet in the Commission’s briefing note for the EPSCO meeting.
Article 97 MDR – the silver bullet bridging measure?
Right after the EPSCO meeting MDCG 2022-18 dropped, the bridging measure that the Commission referred to. ‘Bridging measure’ has a degree of optimism to its name right? We go from one place to the other where we were unable to do so before, and when we get to the other place we will be where we want to be.
The question is how much the Article 97 MDR option is going to help patients and industry. The problem is that the Article 97 MDR process is most likely understaffed at competent authorities, which means that there will be – again – significant congestion in the system. A telling sign of how well all of this is under control is that the Dutch competent authority IGJ put up a webpage with a huge ‘article 97 guidance for NL coming soon’ cliffhanger some time after MDCG 2022-18 was published. You might think that a clear pathway for these applications would be a matter of urgency and that competent authorities when working on MDCG 2022-18 in the MDCG would have seen this coming and had their local pathways ready – apparently not. But, the Commission proposal (discussed above) may still influence things on this point.
As I have discussed, MDCG 2022-18 leaves a lot of open points (e.g. as regards SMEs and MDD certificates that have already expired) and therefore lots of potential for national divergence. In this regard it is unfortunate that the choice was made for an MDCG document and not for an implementing act under Article 97 (3) MDR, because this leads to less responsibility and more potential divergence – and l 024-mdr-danger-zone-and-outlines-of-a-potential-solution-in-mdcg-2022-11/]). This is the bridging aspect.
The MDCG 2022-18 position paper in its newest version (it has been changed without notice or version control after the initial making available for download on 9 December) contains an annex with a checklist of what to submit for an Article 97 (1) exemption. And now let’s hope that the competent authorities have sufficient headcount available to process these applications in a timely manner.
IVDR – a similar disaster in slow motion
If there is one thing clear it is that the IVD industry seems to have learned absolutely nothing from the dire situation of manufacturers under the MDR that was caused by going all in on maximum use of the grace period and waiting until the very last day of the transitional regime with MDR conformity assessment applications (all these 26 May 2024 certificates that led to many manufacturers also kicking the can down the road as far as possible and starting conformity assessment too late – aggravated by notified bodies not being available). IVD manufacturers seem to be doing exactly the same now after the early 2022 change to the IVDR grace periods. The capacity problem is different for the IVDR however, at least at the moment: beginning 2022 the transitional regime for the IVDR has been changed as to implement staggered grace periods for different risk classes and by the end of 2022 the number of IVDR conformity assessment applications had dropped to the point that even the few notified bodies notified for the IVDR start to publicly advertise available slots for conformity assessment.
Another problem under the IVDR is the widespread resistance of health institution laboratories against compliance with the in-house produced devices regime under article 5 (5) IVDR. MDCG guidance on the in-house produced devices regime is still – as it has been for a very long time – forthcoming. I see also a reluctance on the part of market surveillance authorities to act against non-compliance by health institutions after the first parts of Article 5 (5) IVDR became applicable on 26 May 2022, which they should take care to not see lead to discriminatory market surveillance between CE marked devices and in-house produced devices. In the end, the GSPRs apply to fully to all devices that are deployed clinically on patients outside performance study, regardless of where the device is developed. Of course it does not help here that the MDCG guidance for in-house produced devices still has not been issued, making it hard for competent authorities to enforce and for health institutions to comply.
“important that the MDCG, with the support of the Commission, pursue its work to implement also the remaining actions”.
Information note from the Commission for the EPSCO meeting
Indeed, that’s an understatement. Member states in the MDCG for example totally control themselves whether medicines agencies of the member states cooperate sufficiently in the conformity assessment of combination products (point 19 of MDCG 2022-14). It is vital that the MDCG and respective member states continue to be part of the solution rather than of the problem by implementing not only the 19 MDCG 2022-14 points, but also more generally be the best authorities and coordinating body that they can be. Let’s not forget that behind every device that does not make it to market or that has to be withdrawn from the market due to certification issues there are patients that may not get the medical care they need or to the standards we pride ourselves on in Europe.
To make this very concrete and specific: for me this is as critical that my family members that are dependent on pacemakers and ICDs will likely not receive the latest model with the latest algorithms available if they are up for a replacement in the near future, and will literally be missing out on medical innovation and potential increase in standard of care that can benefit them for a better outcome. And all of this only because of bad legislative choices, an understaffed notified body re-notification process and a generally badly managed transition period. And the worst is that these choices were made to solve a problem (fraud) that you cannot solve this way, because the MDR and IVDR can in no way prevent a manufacturer intent on committing fraud to do so.
However, the other stakeholders have a role to play in making the system function as well.
Notified bodies have a role to play in the roll-out of MDCG 2022-14. I see increasingly erratic behavior around planning of assessments and audits, making it absolutely impossible for manufacturers to predict the time of conformity assessment. In addition, I see notified bodies offer red carpet conformity assessment programs that they sometimes really fail to deliver on. The tragedy there is also that SMEs generally cannot even afford these premium programs. Some of the decisions I see notified bodies take would really be at odds with principles of good administration (such as sometimes making very impactful and costly (for the manufacturer) clerical errors and for some reason not being able to correct them immediately), by which the competent authorities are bound (Article 99 MDR / Article 94 IVDR). It appears that notified bodies do not always seem aware of the fact that they are exercising delegated state authority concerning market access, the exercise of which should be subject to good administrative practice. In that regard it remains forever puzzling to me as a lawyer why Annex VII, 4.8 on decisions and certifications only describes that the procedures should be documented but not that they should be applied in accordance with the principles of good administrative practice, which is the very least you would expect if delegated state authority is applied. ISO 17021:2015 does not provide for this either, describing only a need for documented procedures but not for good administrative practice. And don’t get me started about the possibilities of legal review / appeal of notified body decisions. In that respect it would be useful to do the thought experiment discussed below: what if the government agency for medicines marketing authorizations would act that way? And you would have no viable means to challenge that in court? Would that be acceptable?
Finally, manufacturers do not always put in their best effort either. Regulatory departments may be under-resourced (because it only concerns market access of core business, so why would that be important), are sometimes undertrained (leading to sub-standard conformity assessment applications that do not make it to validation and actual start of the assessment) or management decides to postpone submissions for MDR or IVDR conformity assessment because ‘there still is time’. Not a good idea at this time for the Union market.
Thought experiment with medicines regulation
EU pharmaceutical law is currently up for a major revision, and it is my firm expectation that this will somehow be managed a lot better than the MDR and IVDR legislative changes. For the life of me I cannot understand why we accept such stunning underperformance of the EU regulatory system for medical devices. In discussions I often invite people to do the thought experiment: “What if this happened in pharmaceutical products regulation?”. Usually the sad answer is: nobody would accept this and the world would be too small to fit all the outrage in.
Maybe it would be good for the MDCG, the Commission and the member states to do this thought experiment, it might give them a bit more of a sense of urgency and purpose. Member states and the Commission might provide more resources to make the medical devices regulatory system work.
Rolling Plan and ‘planned’ guidance
According to the Rolling Plan we have several things to look forward to in 2023:
an implementing act on designation of EU reference labs for the IVDR (possible as of 2020, better late than never),
entry into force of Commission Delegated Regulations amending Regulation (EU) 2017/745 and Regulation (EU) 2017/746 as regards the frequency of complete re-assessments of notified bodies (one of the actions from MDCG 2022-14),
updated harmonised standards (now that would be nice and very much needed), and
a Commission Delegated Regulation on UDI assignment criteria for highly individualised devices (contact lenses).
In terms of MDCG guidance under development it’s kind of remarkable that no guidance whatsoever has been slated for 2023. I guess this means that we might interpret this as that all the guidance that was slated for 2022 but was not delivered will be delivered in 2023? That’s a bit of a cheeky statement because literally every MDCG guidance document announced but not yet delivered yet was slated to be delivered in 2022. So we’ll need to see how this goes, the MDCG being the MDCG, sometimes taking years for a guidance document.
Time to restore trust in the EU medical devices regulatory system in 2023
I think that 2023 will be the year in which the MDR will need to prove that the regulation (and especially market access component since legacy devices are not grandfathered) is fit for purpose and in which the EU must restore trust in the EU medical devices market access system, because I see all around me that it is at an all time low. For that we need a Commission proposal in January that works, competent authorities providing a reliable and quick article 97 MDR pathway that works and further roll-out of the MDCG 2022-14 points is needed. And these three things need to work together well.
Already many large and small companies have gotten quite disillusioned and are moving away from an ‘EU first’ market access strategy. It may take years to regain this trust, but 2023 is the year in which the trend of trust will either slowly start to climb up again or will plummet further.
For the IVDR the main issue will be to avoid that the same mistakes as under the MDR are made, perpetuating the same problems and leading to the same problems as under the MDR. Also industry has a role to play there, by utilizing the available notified body capacity as much as possible and not adopting a waiting and seeing approach. And notified bodies can help by being ideal wielders of delegated state authority.
So happy new year my dear readers! Let’s cross our fingers for 2023 (especially if you’re a patient in the Union dependent on medical technology) and let’s all do our best to be part of the solution rather than of the problem. Because in the end the actual health of actual people depends on it.